Spontaneous abortion: Nursing
1,008views
Notes
| SPONTANEOUS ABORTION | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Spontaneous abortion, commonly referred to as a miscarriage, is the loss of pregnancy by natural causes before a gestational age where the fetus can live outside the uterus. This is generally classified as any time before 20 weeks of gestation or when the fetus is 500 grams or 1.1 pounds, or less. Loss of pregnancy at 20 weeks gestation and beyond is called stillbirth or fetal death. Three types of spontaneous abortion include incomplete, complete, and missed.
Now let's quickly review the physiology of gestational development. First, fertilization takes place in the ampulla of one of the two fallopian tubes, which is a muscular passageway where the egg moves from its starting position in the ovaries to the uterus. After about 6 to 8 days, the zygote begins implanting into the uterus. During the first four weeks of pregnancy, the four fetal membranes develop. These are the chorion and the amnion, as well as the yolk sac and the allantois. Of these, the allantois gets incorporated into the umbilical cord, the amnion becomes the amniotic sac, the chorion contributes to the development of the placenta, while the yolk sac eventually shrinks and disappears. Now, the placenta, along with two umbilical arteries and one umbilical vein, is the main exchange point between the pregnant individual and the developing fetus throughout pregnancy. This serves as an exchange point between the pregnant individual and the fetus.These structures allow for an exchange between the pregnant individual and the fetus, where nutrients and oxygen rich blood pass to the fetus, and waste products pass from the fetus.
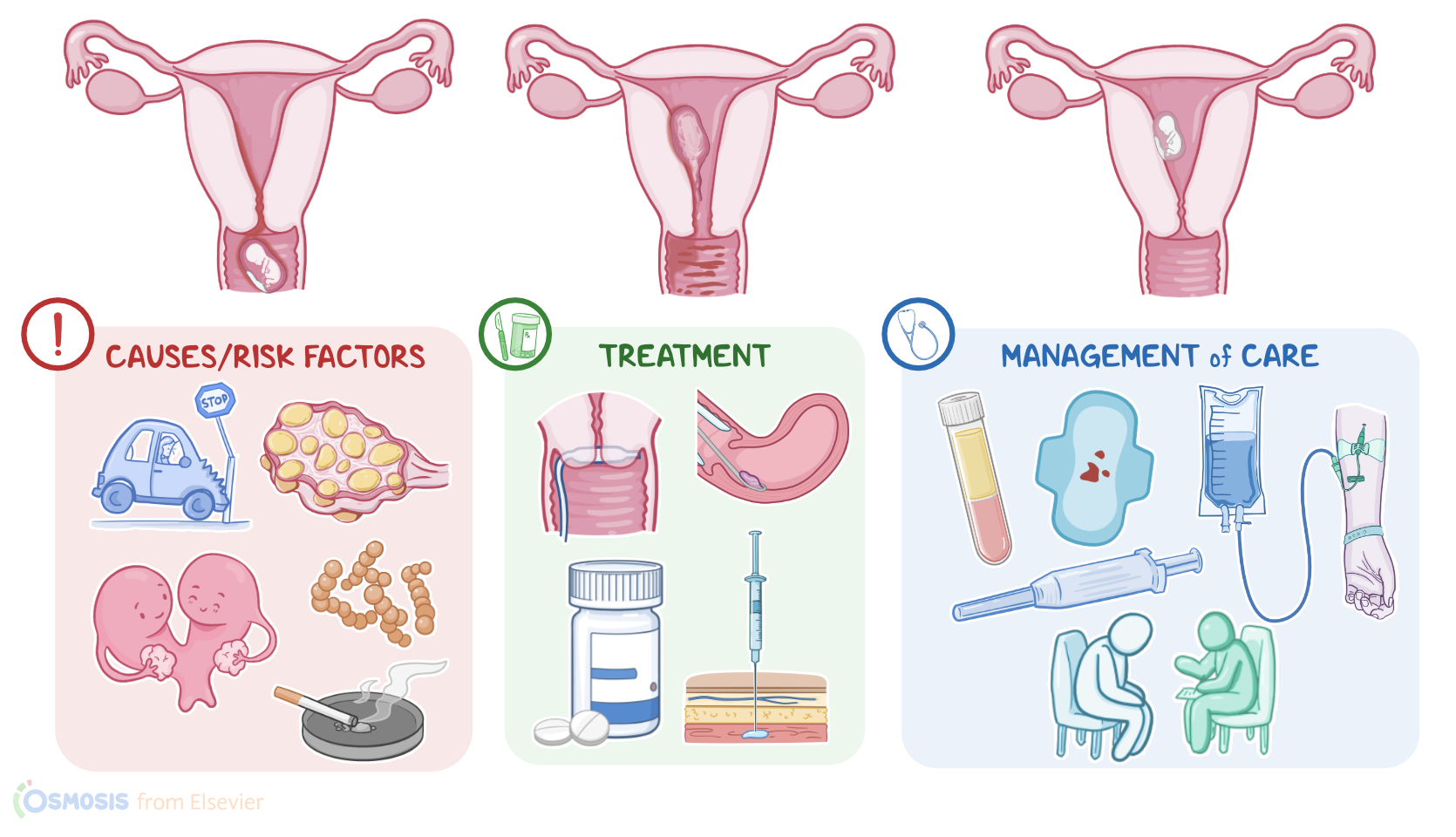
Alright, now, there are many causes for a spontaneous abortion, the most common of which is a fetal chromosomal disorder. Often, this chromosomal disorder is a trisomy where the fetus has 3 copies of a specific chromosome instead of 2. Certain trisomies like, 16 and 22, are incompatible with life. A spontaneous abortion can also occur because of maternal conditions, like endocrine disorders, infections, uterine conditions like uterine fibroids or endometriosis, or immune disorders like antiphospholipid syndrome where the body attacks certain cell membranes.
Risk factors for having a spontaneous abortion include advanced maternal age, previous pregnancy loss, maternal chronic disease, infections, and structural uterine abnormalities. Other factors include significant trauma, underlying endocrinological or gynecological disorders, and exposure to substances like tobacco, alcohol, drugs or environmental contaminants; as well as a history of spontaneous abortion.
So, the pathology varies based on the cause and type of spontaneous abortion. Typically, with a complete or incomplete abortion, the uterus contracts to expel the contents inside the uterine cavity. With a complete spontaneous abortion, all contents are expelled; while with an incomplete abortion, some contents, like the placenta or fetal membranes, depending on gestational age, can be retained. Finally, with a missed spontaneous abortion, no uterine contents are expelled. Sometimes a missed abortion is also called a “silent” abortion, when it causes no signs or symptoms.
Complications of a spontaneous abortion include infection leading to septic abortion, disseminated intravascular coagulation or DIC, hypovolemic shock, as well as trauma to the uterus from surgical intervention.
Now, the clinical manifestations also vary by type, but with complete and incomplete abortions, there’s typically abdominal pain, cramping and vaginal bleeding; on pelvic examination, there’s an open cervix. If the abortion occurs secondary to an infection, there can also be a fever and purulent vaginal discharge; and hypotension can occur if the infection progresses to septic shock. Now, with a complete spontaneous abortion, after complete expulsion of uterine contents, uterine bleeding typically stops and the cervix closes back up. With incomplete spontaneous abortions, on the other hand, following partial expulsion, there’s increased uterine bleeding along with severe abdominal cramping, and continued cervical dilation. When there is significant blood loss during the expulsion of the products of conception, then hypovolemic shock can occur, causing symptoms like weakness and dizziness. In missed spontaneous abortion, the cervix is usually closed and the early pregnancy symptoms, such as nausea and breast tenderness, disappear and the uterus stops growing. Vaginal bleeding may or may not occur.
Diagnosis of spontaneous abortion starts with the client’s history and physical assessment, followed by an ultrasound and laboratory testing. This includes a CBC, which can show leukocytosis with an infection. hCG and progesterone levels, which normally rise during pregnancy and fall following a spontaneous abortion, can also be determined. Cultures from various sites, including blood cultures, can also be taken when an infection is suspected.
Treatment for spontaneous abortion can also vary by type. If a complete abortion is confirmed, and the client is stable, then typically no treatment is needed. For an incomplete or missed abortion, the remaining intrauterine contents may come out on their own, but medications that induce uterine contractions, like vaginal prostaglandin or misoprostol; as well as interventions like dilation and curettage, or D&C, can be required. After the abortion, clients that are RH negative should receive Rho(D) immunoglobulins to prevent the development of anti-D antibodies that could cause trouble in future pregnancies with a potentially RH positive fetus. A client who experiences any additional hemorrhaging may also be given oxytocin intravenously followed by methylergonovine intramuscularly. Finally, many clients also need emotional support during this time and may wish to speak with a counselor.
Alright, let’s move on to the care you’ll provide for a client experiencing a spontaneous abortion. Your priority goals of nursing care include maintaining fluid balance, preventing infection, managing pain, and providing emotional support.
Key Takeaways
Spontaneous abortion, also known as a miscarriage, is the loss of a pregnancy before the 20th week of gestation. Spontaneous abortion can be complete, incomplete, or missed. With a complete spontaneous abortion, all contents are expelled; while with an incomplete abortion, some contentS like the placenta or fetal membranes, depending on gestational age, can be retained. If it is a missed spontaneous abortion, no uterine contents are expelled.
Symptoms of spontaneous abortion can include vaginal bleeding, cramping, and the passing of tissue from the vagina. In missed spontaneous abortion, people may experience no symptoms and may be discovered during a routine prenatal ultrasound or exam. Diagnosis involves clients' history and physical assessment, followed by an ultrasound and laboratory testing, including a complete blood count, hCG and progesterone levels, and possible cultures of blood or vaginal discharge samples.
Treatment depends on the type of abortion and can involve medications that stimulate uterine contractions or control the bleeding, conservative management, or surgical procedures like dilation and curettage. Rh-negative clients should be administered Rho(D) immunoglobulin after the abortion. Priority goals of nursing care include maintaining fluid balance, preventing infection, managing pain, and providing emotional support. Client and family teaching focuses on teaching them about their condition and treatments, self-care, and when to seek medical assistance.