Syndrome of inappropriate antidiuretic hormone (SIADH): Nursing process (ADPIE)
Notes
| SYNDROME OF ANTIDIURETIC HORMONE (SIADH) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Jamal Hashim is a 68-year-old male client who presents to his primary care provider’s office along with his wife, Admira.
Jamal was recently diagnosed with depression and has been taking the selective serotonin reuptake inhibitor, or SSRI, sertraline, for the past 3 weeks.
Today, Jamal reports that he’s been experiencing intermittent forgetfulness, headache, lethargy, muscle weakness, and decreased urine output.
Laboratory results showed a serum sodium level of 124mEq/L. His SSRI is discontinued and Jamal is admitted to the medical unit for continued monitoring and treatment of syndrome of inappropriate antidiuretic hormone.
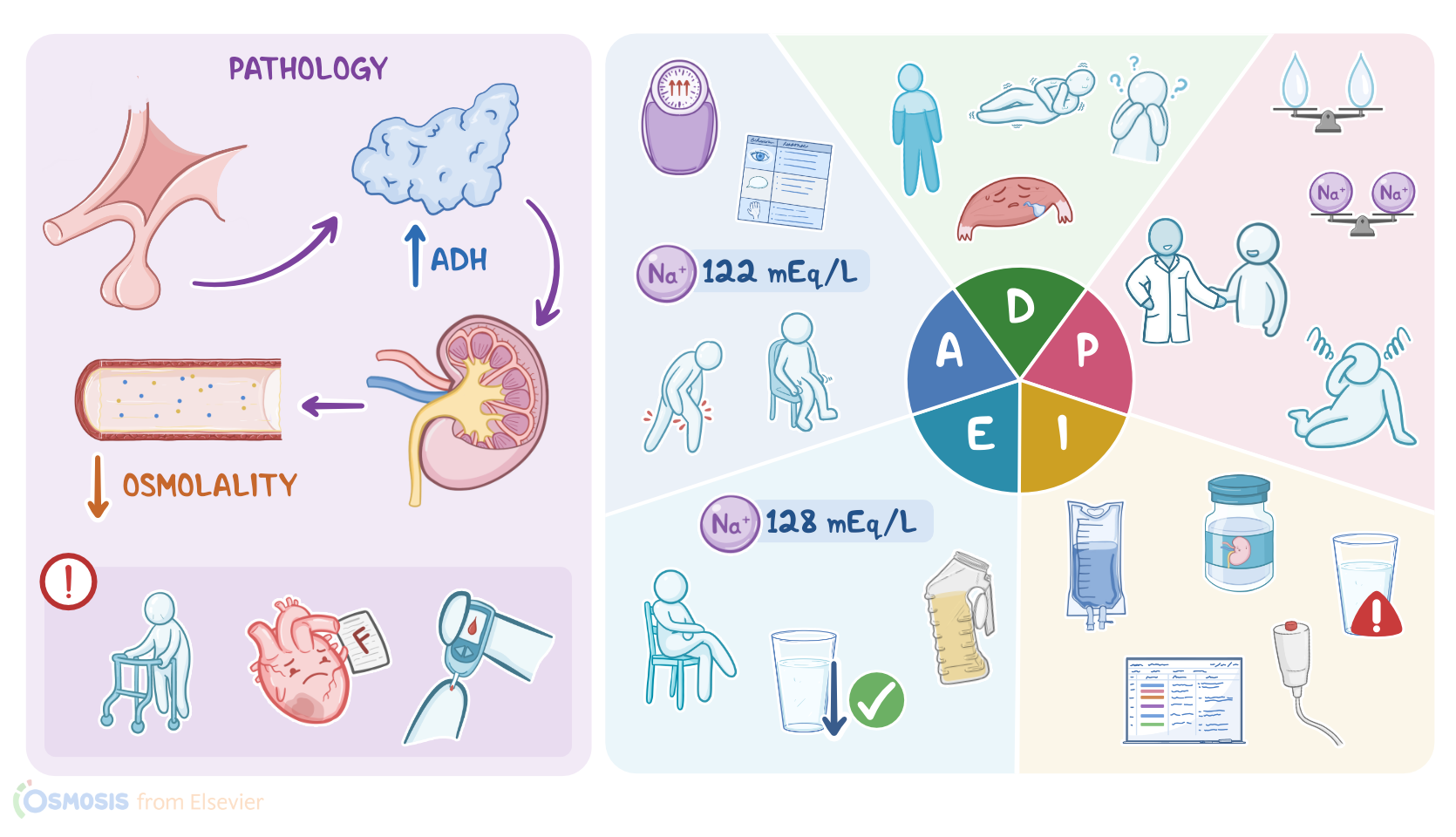
Syndrome of inappropriate antidiuretic hormone secretion, or SIADH for short, is a condition where the body produces too much of the hormone ADH, also called vasopressin, leading to decreased blood osmolality, which refers to the concentration of dissolved particles like sodium and other electrolytes.
The normal blood osmolality value is between 285 and 295 milliOsmoles per kilogram.
Now, ADH is the primary hormone that regulates fluid balance in the body, and is normally produced by the hypothalamus and stored in the posterior pituitary, which are both located within the brain.
To do this, the hypothalamus contains osmoreceptors, which are able to sense the osmolality of the blood.
When a person is dehydrated, for example, osmolality increases, so osmoreceptors sense this and, in response, stimulate the pituitary to release the stored ADH into the blood.
ADH then travels to the kidneys to decrease water excretion in urine, and increase water reabsorption back into the blood, to help restore normal blood osmolality.
In addition, osmoreceptors trigger the sensation of thirst. After the person drinks water, the osmolality returns to normal, and ADH secretion stops.
Okay, now SIADH can have several important causes. The first one is paraneoplastic syndrome, where a tumor outside the brain secretes ADH. This is especially common in clients with small cell lung carcinoma.
Other pulmonary diseases, such as pneumonia and chronic obstructive pulmonary disease or COPD, can also temporarily lead to SIADH, but the exact mechanism is unknown.
Other causes include surgeries of the central nervous system or head trauma that may damage the pituitary, which can cause stored ADH to be released.
Finally, SIADH can be caused by certain medications, including seizure medications like carbamazepine, antidepressants like selective serotonin reuptake inhibitors, or SSRIs, certain antidiabetic medications, as well as antihypertensive medications like thiazide diuretics, chemotherapeutics like cyclophosphamide, and analgesic medications like NSAIDs.
Also, several risk factors can increase the risk of SIADH, and the most important ones are advanced age, and having chronic conditions, such as epilepsy, heart failure or diabetes mellitus.
Now, with SIADH, the increased ADH leads to increased water reabsorption in the kidneys.
This results in dilutional hyponatremia, where the total amount of body water increases which then lowers the plasma concentration of sodium by dilution.
Hyponatremia typically presents with gastrointestinal symptoms, including abdominal cramps, nausea, and vomiting.
Additionally, hyponatremia can lead to muscle weakness, as well as altered mental status, such as restlessness, irritability, and confusion.
SIADH can also cause some severe complications. The most dangerous one is cerebral edema, which occurs due to excessive accumulation of fluid in the brain, leading to increased intracranial pressure and can cause seizures, coma, and even brainstem herniation and death.
Diagnosis of SIADH generally involves blood tests showing decreased blood osmolality and hyponatremia, which is when sodium goes below 136 mmol/L.
Diagnosis is supported by a urine test showing increased urine osmolality.Treatment of SIADH is based on fluid restriction.
Additionally, to excrete the extra water, clients may take medications, such as loop diuretics like furosemide, or vasopressin receptor antagonists, such as tolvaptan.
Finally, salt tablets and intravenous administration of hypertonic saline can help correct the hyponatremia.
It’s important to note that hyponatremia should be corrected slowly in order to prevent osmotic demyelination syndrome, which is associated with severe neurological consequences. Finally, whenever possible, the underlying cause should be treated.
Jamal and Admira have just been admitted to the medical unit, and you begin your assessment by noting Jamal is orientated to his surroundings, he is able to answer all your questions appropriately, but he occasionally repeats questions that he already answered.
Key Takeaways
Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is characterized by excessive release of antidiuretic hormone from the posterior pituitary gland or another source. The increase in fluid retention often results in dilutional hyponatremia in which the plasma sodium levels are lowered. SIADH may present with euvolemic hyponatremia with continued urinary sodium excretion. Urine osmolality is usually higher than serum osmolality. Very low serum sodium levels can lead to cerebral edema or seizures. Other symptoms of SIADH include fatigue, confusion, muscle weakness, nausea, vomiting, lack of appetite, and weight loss. Treatment usually involves fluid restriction, salt tablets, IV hypertonic saline, diuretics, and drugs like conivaptan, tolvaptan, or demeclocycline.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Hyponatremia in the emergency department" Am J Emerg Med (2022)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Approach to the Patient: Hyponatremia and the Syndrome of Inappropriate Antidiuresis (SIAD)" J Clin Endocrinol Metab (2022)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)
- "Syndrome of Inappropriate Antidiuresis: From Pathophysiology to Management" Endocr Rev (2023)
- "Health Assessment for Nursing Practice, 7th edition" Elsevier (2021)