Systemic lupus erythematosus (SLE): Nursing
Introduction0:00–0:35
Systemic lupus erythematosus, or simply SLE or lupus, is a chronic autoimmune disease that affects multiple systems, mainly the skin, joints, and serous membranes.
SLE is progressive, meaning that it gets worse over time with alternating periods of remission and exacerbation. A less common type of lupus particularly affects the skin, called cutaneous lupus erythematosus, or CLE for short.
Clients with this condition eventually develop a full-blown SLE over time. Now, let’s quickly recap the physiology of the immune system, which protects the body from harmful agents.
Physiology0:35–2:19
This can be done with the aid of immune cells, including macrophages and lymphocytes. So, let’s imagine that a foreign particle enters the body, it will be faced by macrophages, which swallow this harmful agent and break it down, leaving a small particle called an antigen.
The macrophage then presents this antigen on its surface for another type of immune cells to recognize, called T lymphocytes.
Types of T lymphocytes include cytotoxic T lymphocytes, which fight against intracellular pathogens and cancer cells by initiating cell death; as well as T helper cells, which activate another type of lymphocytes, called B lymphocytes.
Once activated, B lymphocytes can differentiate into plasma cells or memory cells. Plasma cells produce antibodies.
These bind to antigens found on the surface of the pathogen, producing immune complexes. So, an antibody tags the pathogen for other immune cells to recognize.
In contrast, memory cells monitor the body for the same antigen, and when the pathogen visits the body again, these cells convert to plasma cells, and start producing antibodies to fight this pathogen even faster than the first exposure.
During development, the immune cells learn how to skip the antigens found on the surface of body cells and not react to them, called self-tolerance.
This is the main function of another type of T lymphocytes, called regulatory T cells, which suppress the immune system to maintain self-tolerance.Now, the exact cause of systemic lupus erythematosus is unknown, but it’s thought to be multifactorial, involving genetic susceptibility, altered immune system function, and exposure to certain triggers such as cigarette smoke and ultraviolet light.
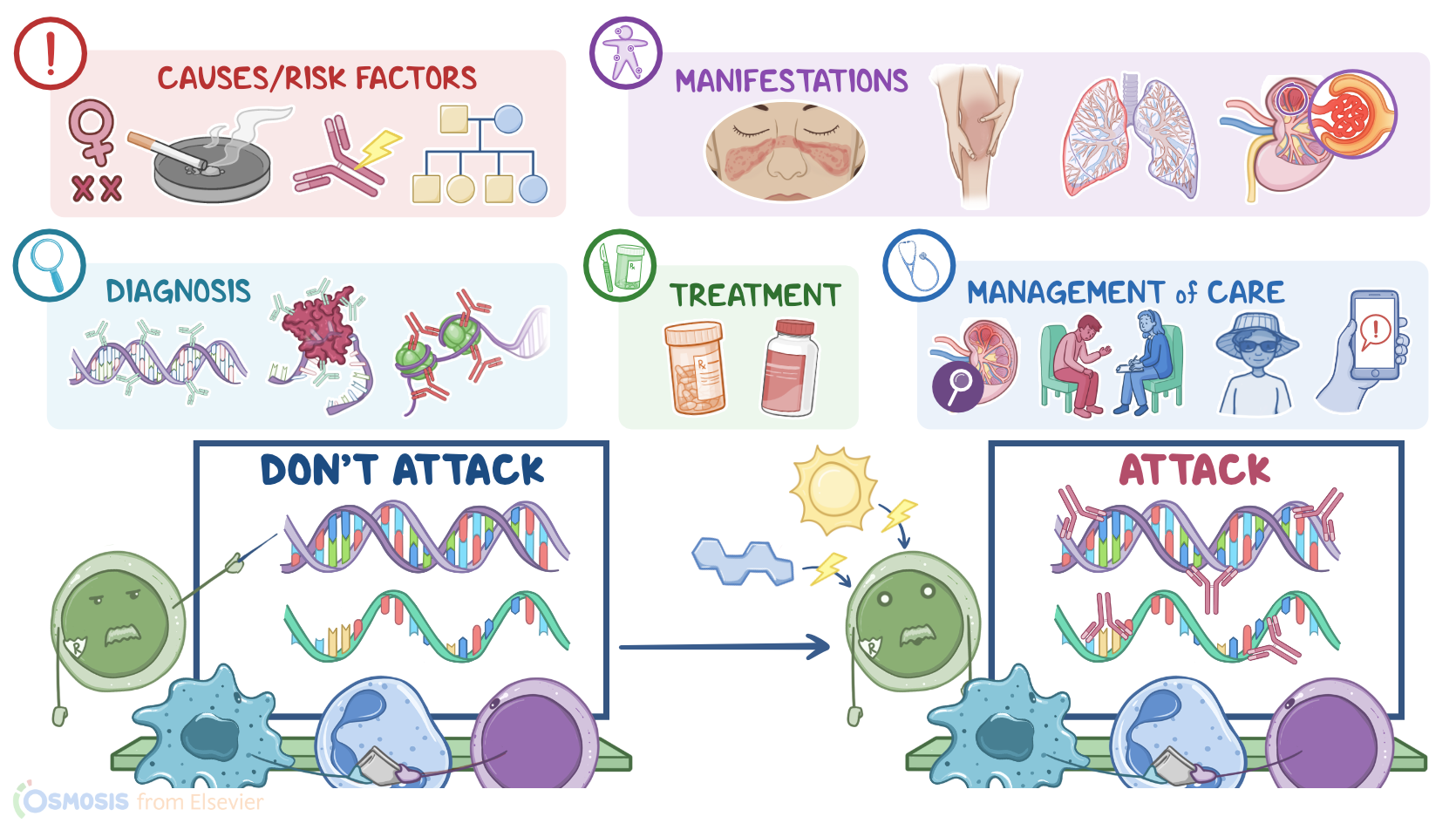
Causes & risk factors2:19–2:47
Lupus is also more common in individuals assigned female at birth, especially during childbearing years; those with a family history of Lupus; and Black, Hispanic, or Asian individuals.Alright, now the pathology of systemic lupus erythematosus starts with a genetically susceptible client, meaning that they have less functional regulatory T cells.
Pathology2:47–4:36
Add a hormonal or an environmental trigger to that, and self-tolerance is lost. This causes the immune system to form auto-antibodies that target nucleic acids, such as DNA or RNA.
Therefore, these auto-antibodies are called anti-nuclear antibodies, or ANA for short. Now, when these ANAs bind to nucleic acids, immune complexes are formed, and these immune complexes eventually precipitate in the walls of blood vessels supplying the brain, heart, skin, kidneys, and joints.
This triggers an abnormal immune response, called type III hypersensitivity reaction, which leads to chronic inflammation of the affected blood vessels and reduced perfusion of the affected organs.
Complications of systemic lupus erythematosus typically arise from the organ damage caused by the disease, or as a side effect of the medications used to treat the disease.
These complications include skin damage, alopecia, and increased risk of coronary artery disease, in addition to end-stage renal disease.
Complications can also arise in the nervous system, including visual changes, anxiety, and depression. Complications of the gastrointestinal system include intestinal obstruction and inflammatory bowel syndrome.
Complications of the reproductive system include pregnancy loss, preeclampsia, and eclampsia. Finally, clients with lupus that receive long-term steroids can develop complications, such as osteoporosis and increased risk for infections.
In terms of clinical manifestations, there are general ones, like fever and weight loss, as well as specific manifestations depending on the organ system being affected.
Clinical manifestations4:36–6:45
Additional skin manifestations include a discoid rash, which is a plaque-like chronic rash in sun-exposed areas, and a general photosensitivity of the skin.
Lupus can also affect the serous, or outer membrane of an organ, so clients can get serositis, which could manifest as pleuritis, or inflammation of the lining around the lungs and chest cavity; as peritonitis, which is inflammation of the lining of the abdomen, or as pericarditis, which is inflammation of the lining of the heart.
In addition to pericarditis, lupus can also cause inflammation of the myocardium, leading to myocarditis, or the endocardium, leading to Libman-Sacks endocarditis, where clumps of fibrin and immune cells form vegetations on the mitral or aortic valve.
The musculoskeletal system is also frequently involved, so clients can experience pain in multiple joints, and myalgia. Next is the urinary system, where lupus can lead to glomerulonephritis, proteinuria, and hematuria.
For neurological manifestations, these include seizures, psychosis, personality changes, and peripheral neuropathy.Gastrointestinal manifestations, such as dysphagia, nausea and vomiting, abdominal pain, and diarrhea, are also common.
Some clients may also experience reproductive manifestations like menstrual abnormalities. Finally, components of the blood can be affected , causing various hematologic disorders, anemia, thrombocytopenia, and leukopenia.
The diagnosis of systemic lupus erythematosus starts with the client’s history and physical examination, followed by diagnostic tests.
Diagnosis6:45–7:51
The gold standard test for the diagnosis of lupus is the ANA test, which measures the amount of antinuclear antibodies in the blood.
Other autoantibodies can also be detected, including anti-dsDNA, anti-Smith, which are actually relatively specific for lupus, and antiphospholipid antibodies.
Additional diagnostic tests are sometimes also performed, including a complete blood count, serum complement levels, electrocardiography, urinalysis, as well as chest x-ray, and x-rays of the affected joints.
Treatment7:51–8:33
Now, treatment of systemic lupus erythematosus depends on the severity of the symptoms and what organ systems are affected, and typically aims at preventing organ damage and minimizing medication toxicity.
So, clients with mild disease often receive NSAIDs, in addition to steroid-sparing medications, such as methotrexate, and antimalarials, such as hydroxychloroquine.
On the other hand, clients with flares or severe disease are typically treated with immunosuppressive medications, such as corticosteroids, cyclophosphamide, and mycophenolate mofetil.
Anticoagulants, such as warfarin, can also be prescribed to prevent blood clots. Alright, now let’s talk about management of care for a client diagnosed with systemic lupus erythematosus.
Management and care8:33–10:16
Your priority goals of care are to control your client’s symptoms, monitor for organ damage, and provide psychosocial support.Begin your assessment by taking your client’s vital signs, assessing their neurological status, and asking about their degree of fatigue and severity of their joint pain.
Report to the healthcare provider if your client has fever, headache, vision changes, or severe joint pain and swelling.
Administer the prescribed medications, including analgesics, corticosteroids, or hydroxychloroquine. Assist your client into a position of comfort, and implement non-pharmacological pain management strategies such as cold packs to the joints; and be sure a referral for physical therapy is in place.
During care, cluster your activities so your client can rest in between interventions. Next, monitor your client for organ damage.
Look for signs of renal damage by checking their latest laboratory test results, monitoring their blood pressure, and observing their extremities and eyelids for edema.
Also insert an indwelling urinary catheter and monitor on their intake and output. Report to the healthcare provider if your client’s blood pressure is elevated, if edema and oliguria are present, or if their lab results show the presence of hematuria, proteinuria, cellular casts, and an elevated BUN and creatinine.
Then, administer the prescribed antihypertensive medication, diuretic, and immunosuppressant, and continue to monitor your client closely.
General client and family teaching10:16–13:00
Alright, let’s move on to general client and family teaching. Begin by explaining that systemic lupus erythematosus is an autoimmune disease, which means that the body’s immune system attacks its own healthy tissue; and many parts of the body are affected.
Then, teach them about their prescribed medications and instruct them to take them exactly as prescribed. Also explain how they work and what side effects they may experience.
Be sure to emphasize the importance of regular checkups by their primary healthcare provider as well as each of the specialists involved in their care.Next, let them know that lupus causes alternating patterns of remission and exacerbations or flares, and teach them strategies to manage their disease and improve their quality of life.
To manage fatigue, recommend that they keep their daily routine as simple as possible, to pace themselves, and allow opportunities for rest between their daily activities.
Remind them of the importance of using stress management techniques, and getting plenty of sleep each night. Also teach them to avoid household chemicals as well as UV light especially between the hours of 11 AM and 3 PM.
When they need to be outside, teach them to wear a wide-brimmed hat and tightly woven clothing, and to use sunscreen with a sun protection factor of at least 50.
Also, stress the importance of avoiding others who are sick, and to talk to their healthcare provider about which vaccinations are right for them.
Also teach them how to decrease the impact of lupus, especially cardiovascular disease, renal disease, and osteoporosis.
Talk to them about how moderate daily exercise can keep their bones strong, their joints mobile, and help keep their weight in check; and discuss dietary modifications with a focus on eating a plant based, high fiber, low fat, and low sodium diet to decrease the risk of dyslipidemia; increasing calcium and vitamin D to promote bone health; and supporting renal function by keeping protein low.
Lastly, if they have a history of smoking, instruct them to avoid any products that contain nicotine or tobacco, such as cigarettes and e-cigarettes, and provide smoking cessation counseling and referrals to help them quit.Finally, instruct your client to seek immediate medical attention if they experience chest pain or pressure, sudden weakness or light-headedness, shortness of breath, if they are urinating less than usual; or if they notice they have increased fatigue, loss of appetite, hair loss, skin rashes, or new sores in your mouth or nose.Alright, as a quick recap… Systemic lupus erythematosus is a chronic, autoimmune disease that affects many parts of the body, most commonly the skin, joints, and serous membranes.
Review13:00–14:36
It is characterized by periods of exacerbation and remission. Although the cause is unknown, risk factors include multiple factors involving genetic susceptibility, altered immune system function, and exposure to cigarette smoke, as well as being assigned female at birth, especially during childbearing years; those with a family history of lupus; and Black, Hispanic, or Asian individuals.
Clinical manifestations depend on the affected organ, and include a classic ‘butterfly rash’ over the cheeks and bridge of the nose, and mucosal ulcers; muscle and joint pain; visual changes; pleuritis; as well as cardiovascular and renal disease.
Diagnosis is based on the client’s history and physical exam and with laboratory tests for antinuclear antibody, anti-dsDNA antibody, and anti-smith antibody.
Treatment involves NSAIDs, immunosuppressive medications, antimalarial medications such as hydroxychloroquine, and corticosteroids.Goals of nursing care include controlling symptoms, monitoring for organ damage, and providing psychosocial support.
Client and family teaching centers on educating about their condition, how it is treated, disease self-management at home, and when to contact their healthcare provider.
| SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below