Urinary retention: Nursing
Notes
| URINARY RETENTION | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| CLINICAL MANIFESTATIONS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Urinary retention is a condition characterized by the inability to completely empty the urinary bladder.
Okay, let’s quickly review some anatomy and physiology. The urinary bladder is a hollow organ that lies behind the pubic bones and pubic symphysis, and it’s superior to the prostate in individuals assigned male at birth or anterior to the vagina in individuals assigned female at birth.
The bladder has a strong wall that’s made up of a urothelium that’s capable of stretching and expansion; as well as a smooth muscle layer called the detrusor muscle, which is able to relax or contract, as needed.
During urination, the bladder empties urine into a muscular tube called the urethra, which extends from the neck of the bladder, or the internal urethral sphincter, to the external urethral sphincter, and carries urine to pass outside our body.
In individuals assigned male at birth, the urethra is long and typically measures about 18 to 22 centimeters. On the other hand, in individuals assigned female at birth, the urethra is short - only about 4 centimeters long.
Now, let’s quickly explain the physiology of urination. First, the urine is formed in the kidneys and passes down into the urinary bladder. As the bladder progressively fills with urine, the urothelium expands and the detrusor muscle relaxes.
When the bladder is almost full, the nerves in the bladder wall send impulses to the micturition center at the brainstem. This activates the micturition reflex, which causes involuntary relaxation of the internal urethral sphincter and contraction of the detrusor muscle, allowing urine to pass down into the urethra. Fortunately, there’s another sphincter that lies just below the internal sphincter, called the external urethral sphincter, which is controlled voluntarily. So, when the individual is ready to urinate, they can voluntarily relax their external sphincter, allowing urine to pass outside the body, and emptying the bladder completely.
Now, there are two main causes of urinary retention: detrusor underactivity and bladder outlet obstruction.
Detrusor underactivity refers to a decrease in strength or duration of bladder contraction. Risk factors of detrusor underactivity include increasing age; neurodegenerative conditions like Parkinson disease, multiple sclerosis, and damage to the spinal cord segments S2, S3, and S4; as well as myogenic diseases; diabetes mellitus; overdistention of the bladder; chronic alcoholism; medications like anticholinergics, and iatrogenic interventions like pelvic surgery and radiation.
On the other hand, bladder outlet obstruction refers to a blockage at the lower part of the bladder or at the urethra. Risk factors for a bladder outlet obstruction include urethral stricture or mass; bladder stones; prostate enlargement due to benign prostate hyperplasia; and pelvic organ prolapse.
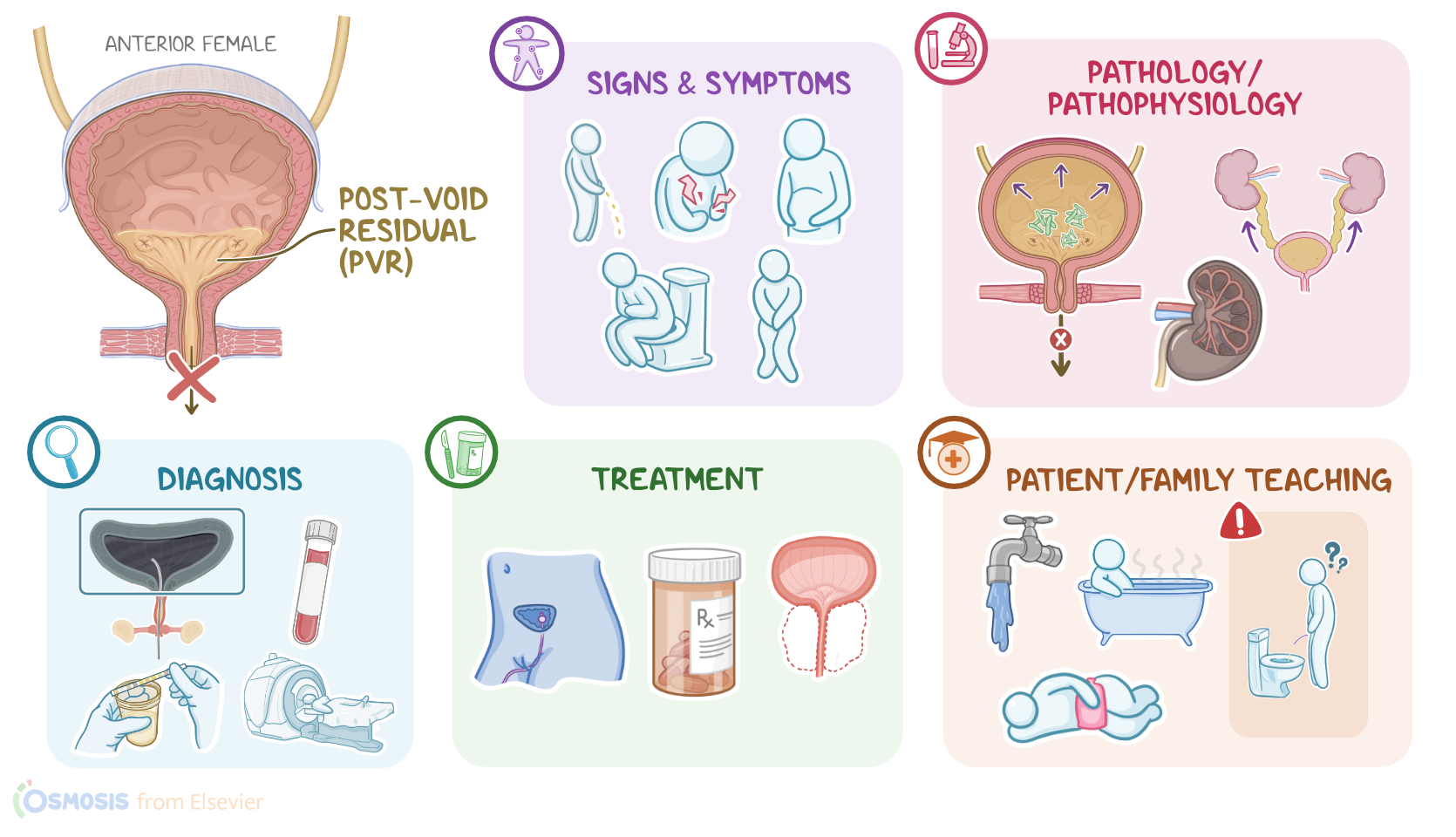
Now, regardless of the underlying cause, the pathology of urinary retention develops when the client is unable to completely empty their bladder. As a result, a residual volume of urine remains in the bladder, and this is called post-void residual or PVR for short.
Unfortunately, clients with urinary retention may develop a few complications, such as bladder damage from overstretching; as well as overflow incontinence, where the overly full bladder may leak involuntarily. In addition, urinary retention may allow bacteria to stay and replicate in the urinary tract, resulting in urinary tract infections or UTIs like cystitis. Lastly, in severe cases, the urine may even back up into the kidneys, which may ultimately lead to pyelonephritis, hydronephrosis, or even kidney failure.
The clinical manifestations of urinary retention can be acute and have a sudden onset, or chronic with slow and gradual onset. Clients with acute urinary retention typically present with sudden inability to urinate that is usually severe. This can be accompanied by suprapubic pain and discomfort, urgency, and a distended bladder that is often palpable..
On the flip side, symptoms of chronic urinary retention are similar, but milder. These symptoms can be accompanied by hesitancy, or difficulty starting or maintaining the flow of urine; as well as frequency, but only being able to urinate small amounts; and a slow urine stream.
The diagnosis of urinary retention starts with the client’s history and physical assessment. Additional diagnostic tests include measuring the post-void residual by draining the bladder with catheterization or via an ultrasound bladder scan. A normal PVR value lies between 50 and 100 milliliters, whereas a PVR of more than 100 milliliters requires clinical correction and further investigation.
Lastly, the underlying cause of urinary retention can be discovered with additional diagnostic tests, such as imaging or blood tests; while a urinalysis and culture can be performed to rule out complications like a UTI.
The treatment of urinary retention starts with intermittent catheterization or indwelling catheter to relieve the client’s urinary symptoms. Clients may also be prescribed medications like alpha-adrenergic blockers, which act by relaxing the internal urethral sphincter to help relieve the urinary symptoms.
Additional treatment options depend on the onset of the condition. In acute urinary retention, a catheter can be used to decompress the bladder. On the other hand, clients with chronic urinary retention may benefit from two techniques: scheduled voiding and double voiding. In scheduled voiding, clients are asked to void every three to four hours, which can increase the capacity of the urinary bladder; whereas in double voiding, clients are asked to void one first time, then waiting for 20 to 30 seconds, and then void again one second time, which aims at maximizing bladder emptying.
Lastly, the underlying cause of the urinary retention should be treated, when possible. For instance, bladder outlet obstruction can be relieved with surgical interventions, such as prostatectomy in clients with prostate enlargement.