Urinary tract infections (UTIs): Nursing process (ADPIE)
Notes
| URINARY TRACT INFECTIONS (UTIs) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Content Reviewers
Contributors
Alejandra Ramirez is a 38-year-old female who presents to urgent care reporting that she has been experiencing painful urination, and has needed to urinate more frequently and urgently than normal over the past two days.
Ms. Ramirez has a history of type 2 diabetes mellitus.
She is sexually active with no history of sexually transmitted infections.
A urinary tract infection, or UTI, happens when the urinary tract which is made up of upper urinary tract, consisting of the kidneys and the ureters, and the lower urinary tract, bladder, prostate, and the urethra, becomes infected by pathogenic microorganisms.
UTIs are most often caused by an ascending bacterial infection.
Esherichia coli, or E. coli accounts for 75 to 95 percent of all urinary tract infections while other bacteria such as Klebsiella pneumoniae, Staphylococcus saprophyticus, or Proteus mirabilis are also common causes of infection.
Once the bacteria enter the urinary tract, they multiply and colonize the urinary tract, causing inflammation.
Inflammation of the urethra, or urethritis, results in dysuria, which is a symptom of pain or burning during urination.
Inflammation of the bladder, or cystitis, leads to edema of the bladder wall, which can result in suprapubic pain, which is pain felt in the lower abdomen near the bladder, a feeling of bladder fullness, and a need to urinate frequently and urgently.
Bacteria in the urine, or bacteriuria, often results in cloudy, foul smelling urine, while damage to the bladder mucosa can cause blood in the urine, referred to as hematuria.
If bacteria ascend further to the upper urinary tract, pyelonephritis, or inflammation of the ureters and kidneys, can occur, producing pain in the side of the back, or flank pain, also called costovertebral angle, or CVA, tenderness, along with manifestations of a systemic response to the infection, such as fever, chills, nausea and vomiting.
Complications of UTIs include scarring and narrowing of the urethra, called a urethral stricture, and damage to the kidney, which can impair its function.
If the infection spreads from the urinary tract to the bloodstream, it can cause urosepsis, which is a systemic reaction to infection that can lead to shock, organ failure, and death.
The risk of a UTI increases with urinary stasis, which is when the normal flow of urine is obstructed and slowed, and urinary reflux, which is when urine moves backwards from the bladder and up to the kidneys.
Urinary stasis and subsequent reflux can occur when kidney stones block the flow of urine through the ureters, or when an enlarged prostate slows the flow of urine through the urethra.
Likewise, a neurogenic bladder, a condition associated with problems like diabetes mellitus and spinal cord injuries, can slow the flow of urine because the nerves and muscles that help the bladder empty don’t work properly.
Other risk factors include the introduction of pathogens in and around the urinary tract, like with urinary catheterization and sexual intercourse, especially with multiple partners, or any factor that depresses the immune response like with HIV/AIDS and diabetes.
There are also a number of reasons why women are at a higher risk of developing a UTI than men.
First of all, women have a shorter urethra, so bacteria have a much shorter distance to travel to enter the bladder.
Furthermore, during pregnancy, increased progesterone levels and the downward pressure from an enlarged uterus tend to relax and dilate the ureters, increasing the risk of urinary stasis and reflux.
And finally, decreased estrogen during menopause alters the normal genitourinary flora, making the urinary tract more susceptible to infection by pathogens.
Diagnosis of a UTI is most often based on client history, physical examination, and diagnostic tests including urinalysis, which looks at the physical and chemical characteristics of the urine, or urine culture, to determine the number and type of organisms present in the urine.
If a UTI is present, the urine will often look cloudy, have a foul odor, will contain nitrites and leukocyte esterase which indicate the presence of bacteria, and microscopic hematuria.
If there are complications or if there are frequent infections where structural problems of the urinary tract is suspected, a computerized tomography scan, or CT scan, or magnetic resonance imaging, or MRI, may be used to visualize the urinary tract.
UTIs are typically treated with antibiotics such as nitrofurantoin, trimethoprim-sulfamethoxazole, and ciprofloxacin.
Urinary tract analgesics such as phenazopyridine can be used to provide pain relief.
Non-pharmacological interventions include the use of heat therapy on the abdomen and increasing the intake of water to help flush out the urinary tract.
Alright, let’s get back to our client Ms. Ramirez.
You enter her room, introduce yourself, perform hand hygiene and confirm her identity.
As you begin your assessment, you notice that she looks extremely uncomfortable.
When you ask her how she’s feeling, she tells you that she has been having pain and burning when she urinates, and that it feels like she has to go to the bathroom “all the time.”
She is concerned because even though she needs to go to the bathroom frequently, she doesn’t produce very much urine.
You ask Ms. Ramirez how much water she drinks each day, and she tells you she is not sure, though she drinks several cups of coffee each day.
She goes on to tell you she’s had three previous UTIs and that she doesn’t understand why she keeps getting them.
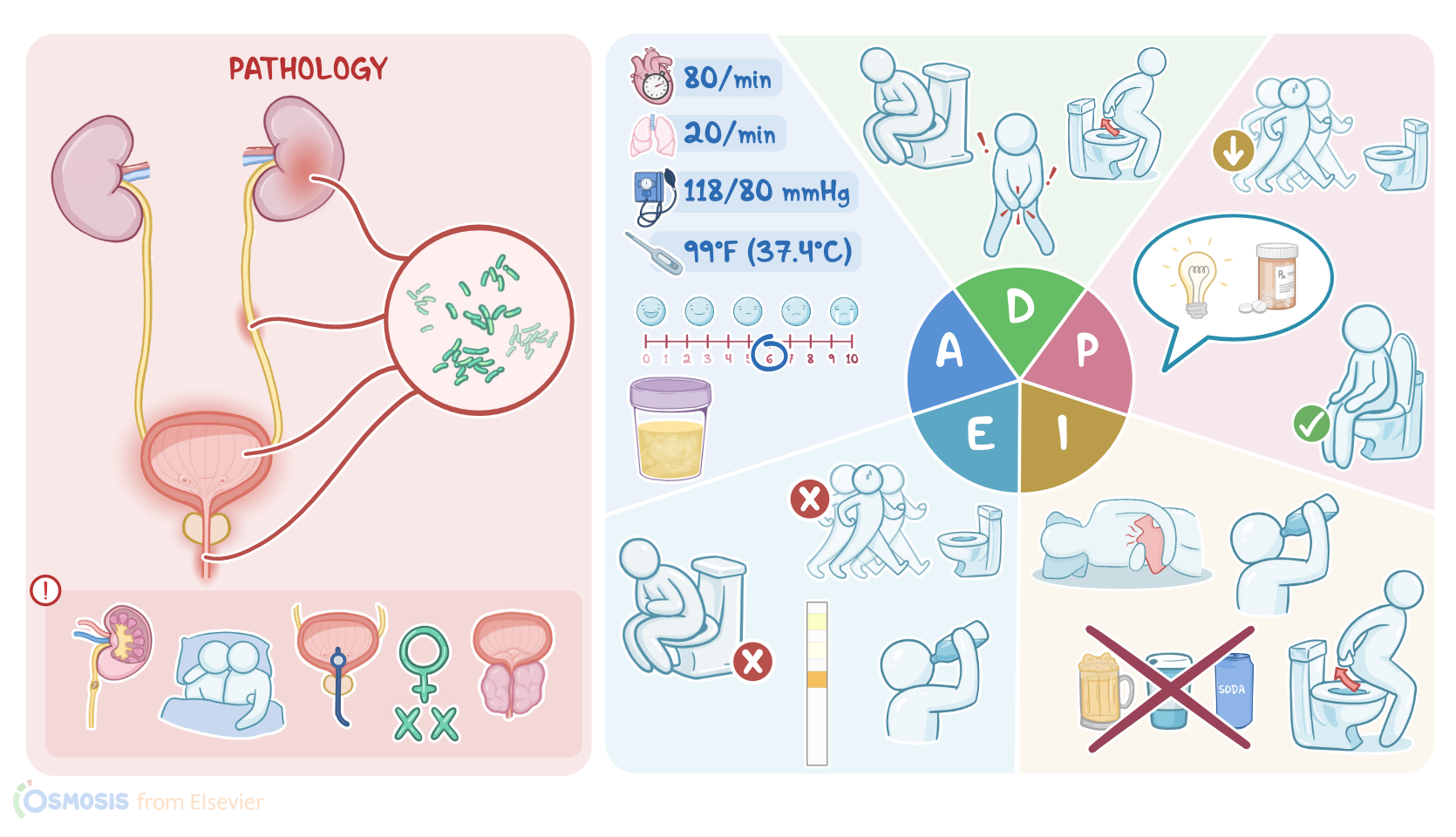
Ms. Ramirez’s vital signs are temperature 99°F or 37.4°C, heart rate 80 beats per minute, respiratory rate 20 breaths per minute, blood pressure 118/80 mmHg, and pain 6/10 when her lower abdomen is gently palpated.