Adrenal insufficiency (Addison disease): Nursing
2,439views
Adrenal insufficiency (Addison disease): Nursing
Acute Final
Acute Final
Notes
| ADRENAL INSUFFICIENCY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
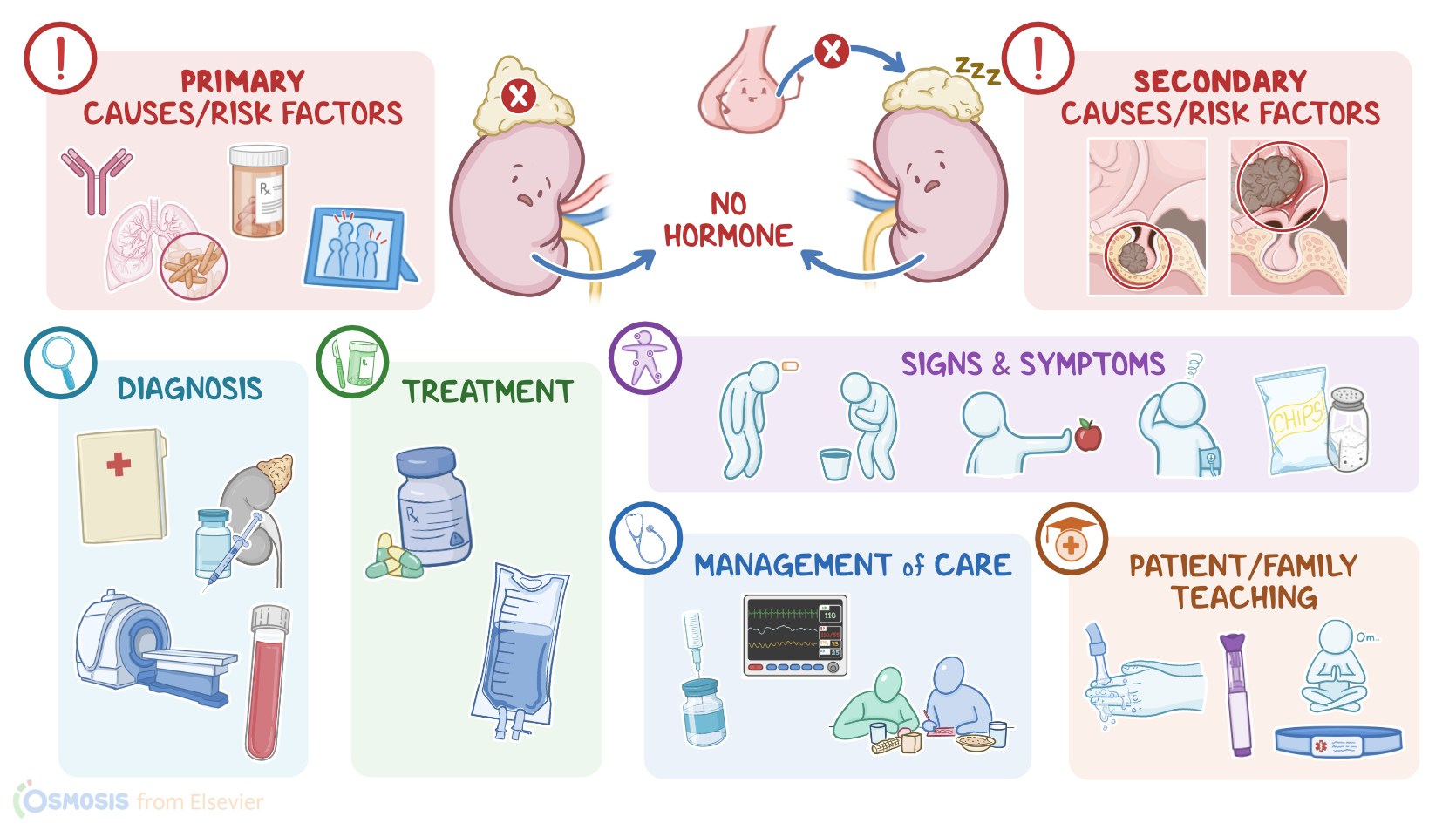
Adrenal insufficiency is an endocrine disorder that happens when the adrenal gland doesn’t produce enough hormones, particularly mineralocorticoids like aldosterone, glucocorticoids like cortisol, and androgens like testosterone. It’s called “primary” when the underlying problem is localized to the adrenal gland itself, which can develop either acutely or chronically, and the chronic form is also known as Addison disease. On the other hand, it’s called “secondary” when the pituitary gland doesn’t stimulate the adrenals enough to ensure adequate cortisol production.
Now, let’s quickly review the anatomy and physiology of the adrenal glands. There are two adrenal glands, one above each kidney, and each one has an inner layer called the medulla and an outer layer called the cortex. Zooming in, the cortex is further subdivided into three more layers, namely the zona glomerulosa, zona fasciculata, and the zona reticularis. And each of their functions can be easily remembered by thinking of the mnemonic Salt, Sugar, and Sex.
So, the outermost layer is the zona glomerulosa, which secretes aldosterone. Aldosterone is part of a hormone system called the renin-angiotensin-aldosterone system. Together, these hormones decrease potassium levels, increase sodium levels, and increase blood volume and blood pressure.
The middle layer is the zona fasciculata, and the cells there make the hormone cortisol as well as other glucocorticoids. The hypothalamus, which is an almond-size structure which sits at the base of the brain, releases corticotropin-releasing hormone, or CRH for short, which acts on the pituitary gland, a pea-sized structure sitting just underneath the hypothalamus. In response, the pituitary gland sends out adrenocorticotropic hormone, or ACTH for short, which stimulates the zona fasciculata to secrete more cortisol.
Now, cortisol is involved in a number of things such as maintaining glucose levels, blood pressure, suppression of the inflammatory and immune response, and it also seems to influence things like mood and memory. Finally, the innermost layer is the zona reticularis, and cells there make sex hormones called androgens, including dehydroepiandrosterone, which is the precursor of testosterone.
So the adrenal glands are involved in testosterone production. In clients assigned male at birth, androgen levels are higher, and they’re responsible for the development of male reproductive tissues and secondary sex characteristics like facial hair and a large thyroid cartilage, also known as “Adam’s apple”.
In clients assigned female at birth, androgen levels are lower, and they are mainly involved in growth, underarm and pubic hair during puberty, and they also influence the sex drive. The exact mechanism for adrenal androgen production is not well understood, but it seems to be stimulated by ACTH.
Okay, now acute primary adrenal insufficiency can arise from Waterhouse-Friderichsen syndrome, which typically occurs as a complication of meningitis, where a sudden increase in blood pressure causes blood vessels in the adrenal cortex to rupture, filling up the adrenal glands with blood and causing tissue ischemia and adrenal gland failure. Acute insufficiency can also occur in clients undergoing adrenalectomy, or surgical removal of the adrenal glands.
Chronic primary adrenal insufficiency is also called Addison disease, and in high-resource countries, the most common cause is autoimmune destruction, where the body’s own immune cells mistakenly attack the healthy adrenal cortical tissues. In the rest of the world, the most common cause of Addison disease is tuberculosis. In this case the infection spreads from the lungs to the adrenal glands, causing inflammation and destruction of the adrenal cortex.
Other causes include metastatic carcinoma, which is where cancer spreads to the adrenal cortex from somewhere else in the body; HIV infection; medications like mitotane that inhibit adrenal cortisol production; and exposure to certain toxins.
Risk factors for developing adrenal insufficiency include the presence of autoimmune disorders, being less than 60 years of age, and having a family history for adrenal insufficiency or autoimmune disorders. On the other hand, secondary adrenal Insufficiency is caused by hypopituitarism, which is when the pituitary doesn’t secrete a sufficient amount of hormones, including ACTH. This is most often caused by large pituitary adenomas, which are benign tumors of the pituitary gland, or by large CNS tumors, like craniopharyngiomas, that compress healthy pituitary tissue.
Other causes of insufficient ACTH secretion is head trauma, radiation, or surgery; as well as Sheehan syndrome, which refers to massive postpartum hemorrhage that causes pituitary ischemia and infarction, ultimately leading to hypopituitarism. Finally, if the cause of hypopituitarism is unknown, it’s called idiopathic hypopituitarism.
Okay, now regardless of the cause, when primary adrenal insufficiency occurs one or more layers of the adrenal cortex get destroyed. When the zona glomerulosa is destroyed, aldosterone levels fall.
When the zona fasciculata is destroyed, cortisol levels fall. Now, cortisol usually has a negative feedback effect on the pituitary gland. As a result when there are decreased levels of cortisol, the pituitary gland becomes overactive. So it ends up secreting more ACTH, as well as more of a hormone that’s an ACTH precursor, called pro-opiomelanocortin. Pro-opiomelanocortin, however, is also a precursor for melanocyte-stimulating hormone, the hormone that stimulates production of melanin, a skin pigment.
In some extreme cases of primary adrenal insufficiency, the zona reticularis can be affected as well, and androgens levels can fall. On the other hand, in secondary adrenal insufficiency, there’s decreased or absent pituitary ACTH production. As a result, there’s no stimulation of adrenal cortisol production.
Okay, now, the clinical manifestations of adrenal insufficiency depend on the layers that are affected. When the zona glomerulosa is affected and aldosterone levels fall, clients may develop electrolyte changes like hyperkalemia, hyponatremia, hypovolemia, hypotension, and metabolic acidosis; as well as hypotension, which can cause symptoms like nausea, vomiting, cravings for salty foods, as well as fatigue, and dizziness that worsens with standing.
When the zona fasciculata is destroyed and cortisol levels fall, clients can feel weak, tired, and disoriented. Also, in clients with primary adrenal insufficiency, increased melanocyte stimulating hormone levels can lead to hyperpigmentation, or darkening of the skin, especially in sun-exposed areas and joints, like the elbows, knees, and knuckles.
Finally, if the zona reticularis is affected, that causes low androgen levels. Now, in clients assigned male at birth, this isn’t as apparent because most of their androgens are actually secreted by the testes. However, in clients assigned female at birth, there can be loss of pubic and armpit hair, as well as decreased sex drive.
Now, clinical manifestations are different in clients with acute primary adrenal insufficiency compared to those with chronic insufficiency. In the acute form, symptoms are usually severe. In contrast, with chronic primary adrenal insufficiency symptoms are more insidious and oftentimes, they can go unnoticed, until a major stressor like a serious injury, surgery, or infection, suddenly causes the symptoms to become really severe.
Key Takeaways
Adrenal insufficiency, also known as Addison disease, is a condition in which the adrenal glands do not produce enough hormones. Symptoms can include weakness, fatigue, weight loss, low blood pressure, and changes in mood and appetite.
Nursing implications for someone with adrenal insufficiency include monitoring their intake of fluids and sodium to prevent dehydration and low blood pressure; providing emotional support; assisting with activities of daily living; and providing education about the condition.
Sources
- "Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care" Elsevier (2020)
- "Lewis's Medical-Surgical Nursing" Elsevier (2022)
- "Saunders Comprehensive Review for the NCLEX-RN Examination" Elsevier (2016)
- "Primary adrenal insufficiency: New genetic causes and their long‐term consequences" Clinical Endocrinology (2019)
- "Therapy options for adrenal insufficiency and recommendations for the management of adrenal crisis" Endocrine (2021)
- "Latent Adrenal Insufficiency: From Concept to Diagnosis" Frontiers in Endocrinology (2021)