Case study - Atrial fibrillation: Nursing
Notes
| CASE STUDY – ATRIAL FIBRILLATION | ||
| KEY POINTS | MY NOTES | |
| INTRODUCTION |
| |
| RECOGNIZING AND ANALYZING CUES |
| |
| PRIORITZING HYPOTHESES, GENERATING SOLUTIONS, AND TAKING ACTION |
| |
| EVALUATING OUTCOMES |
| |
Transcript
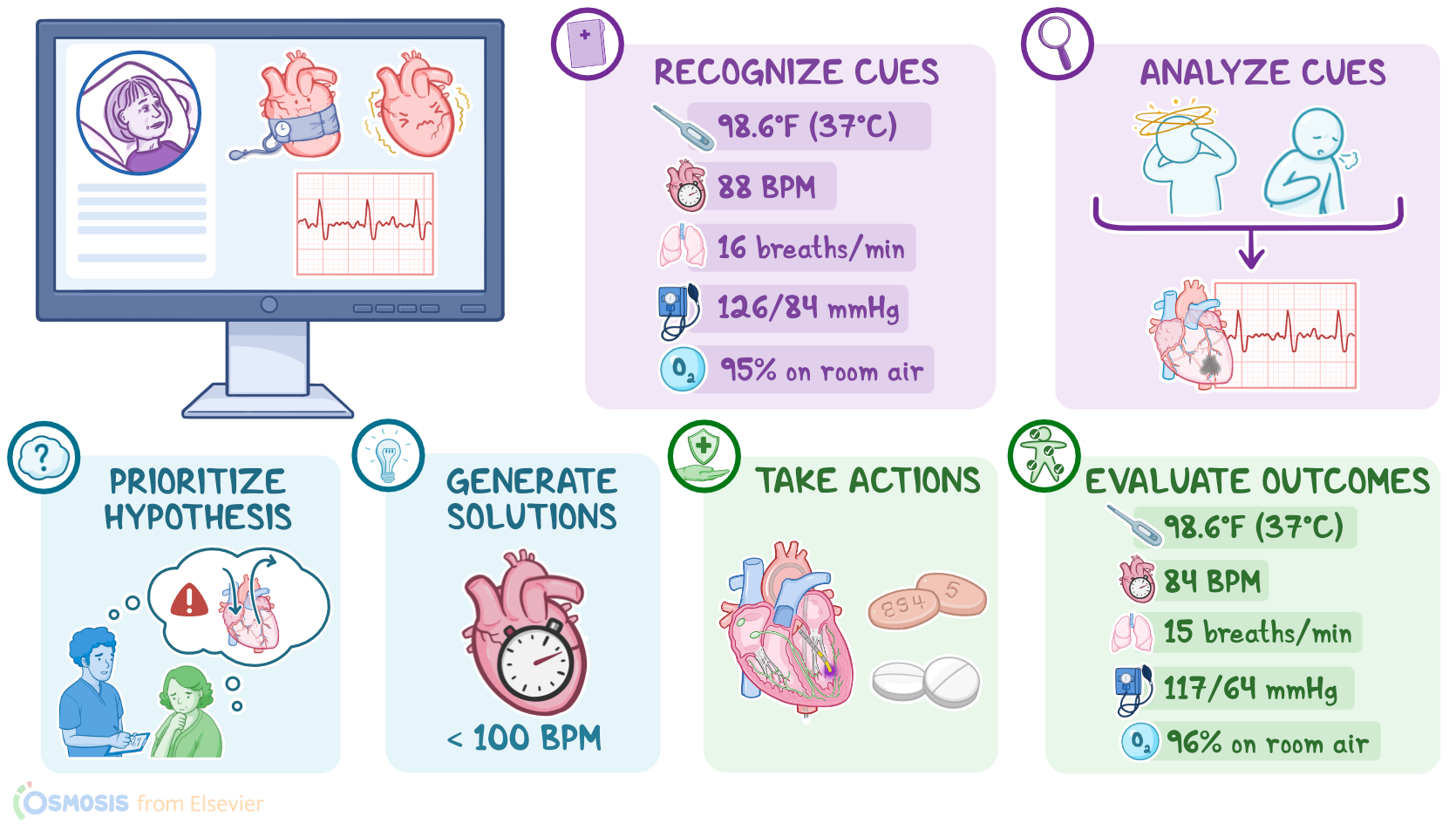
Nurse Jamaal works on an inpatient cardiac unit and is caring for Laurie-Ann, a 64-year-old, with a history of hypertension, who was admitted two days ago after stabilization in the emergency department, or ED, for atrial fibrillation, commonly referred to as Afib, with rapid ventricular rate, or RVR. In collaboration with the registered nurse, RN Eden, Nurse Jamaal goes through the steps of the Clinical Judgment Measurement Model to make clinical decisions about Laurie-Ann’s care by recognizing and analyzing cues, prioritizing hypotheses, generating solutions, taking action, and evaluating outcomes.
First, Nurse Jamaal recognizes important cues, including Laurie-Ann’s vital signs, which are temperature 98.6 F or 37 C, heart rate 88 beats per minute, respirations 16 breaths per minute, blood pressure 126/84 mmHg, and oxygen saturation of 95 percent on room air. Laurie-Ann is awake, alert, and appears comfortable. He also notes that the bedside cardiac monitor shows that she's currently in an irregularly irregular heart rhythm.
Next, Nurse Jamaal analyzes these cues. He reviews the electronic health record, or EHR, and notes that Laurie-Ann came to the ED for dizziness and shortness of breath and was diagnosed with Afib, which is a cardiac arrhythmia that occurs when the regular electrical impulses generated from the heart’s natural pacemaker, known as the SA node, are overridden by disorganized impulses from other areas of the heart. These areas have often been damaged from the effects of conditions like hypertension or coronary artery disease, and the impulses they generate result in many rapid mini contractions, usually between 350 and 600 per minute.
So, instead of one efficient atrial contraction, the atria have a quivering, twitching movement, or fibrillation. The fibrillation causes inefficient emptying from the atria into the ventricles, which means that blood tends to stay in the atria for longer than usual, increasing the risk of clot formation and embolization, where a clot can be pumped from the atria to the ventricles, and then into circulation.
Nurse Jamaal also knows the ventricles respond to the fibrillating atria at an irregular and rapid rate, typically between 100 and 150 beats per minute, and that this rapid response of the ventricles impairs cardiac output and tissue perfusion. Nurse Jamaal recognizes that Laurie-Ann needs management of her atrial fibrillation to support effective cardiac output.
Now, using the information he has gathered, along with Laurie-Ann’s medical history, Nurse Jamaal reports his findings to RN Eden, and together they choose a priority hypothesis of risk for impaired cardiac output.
Then, they generate solutions to address Laurie-Ann’s risk for impaired cardiac output; and they establish the expected outcome that after intervening, Laurie Ann’s heart rate will remain below 100 beats per minute for the duration of the shift.
Nurse Jamaal then takes action to implement these solutions. Nurse Jamaal sees that Laurie-Ann is due for two oral medications, apixaban and diltiazem, and that she’s scheduled for a cardiac ablation later today, to eliminate the abnormal electrical conduction pathways in her heart causing Afib.
Nurse Jamaal then gathers supplies and enters Laurie-Ann’s room.
Nurse Jamaal: Hi Laurie-Ann. I have two different medications for you. One is apixaban, which is an anticoagulant to prevent blood clots, and diltiazem, a channel blocker to regulate your heart rate.
Sources
- "Adult health nursing (9th ed.)" Elsevier (2023)
- "Medical-surgical nursing (8th ed.)" Elsevier (2023)
- "Medical-surgical nursing: Concepts and practice (5th ed.)" Elsevier (2023)