Celiac disease: Nursing process (ADPIE)
Celiac disease: Nursing process (ADPIE)
DEGHAS podle otázek
DEGHAS podle otázek
Notes
| CELIAC DISEASE | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Content Reviewers
Samantha Wilberson is a 29-year-old female client who was admitted to the Medical-Surgical floor during the night. Ms. Wilberson has a history of celiac disease and was directly admitted to the department by her gastroenterologist after a severe bout of watery diarrhea, vomiting, and dehydration. She says the last time she remembers feeling this sick was over a year ago after she had a bad case of the flu.
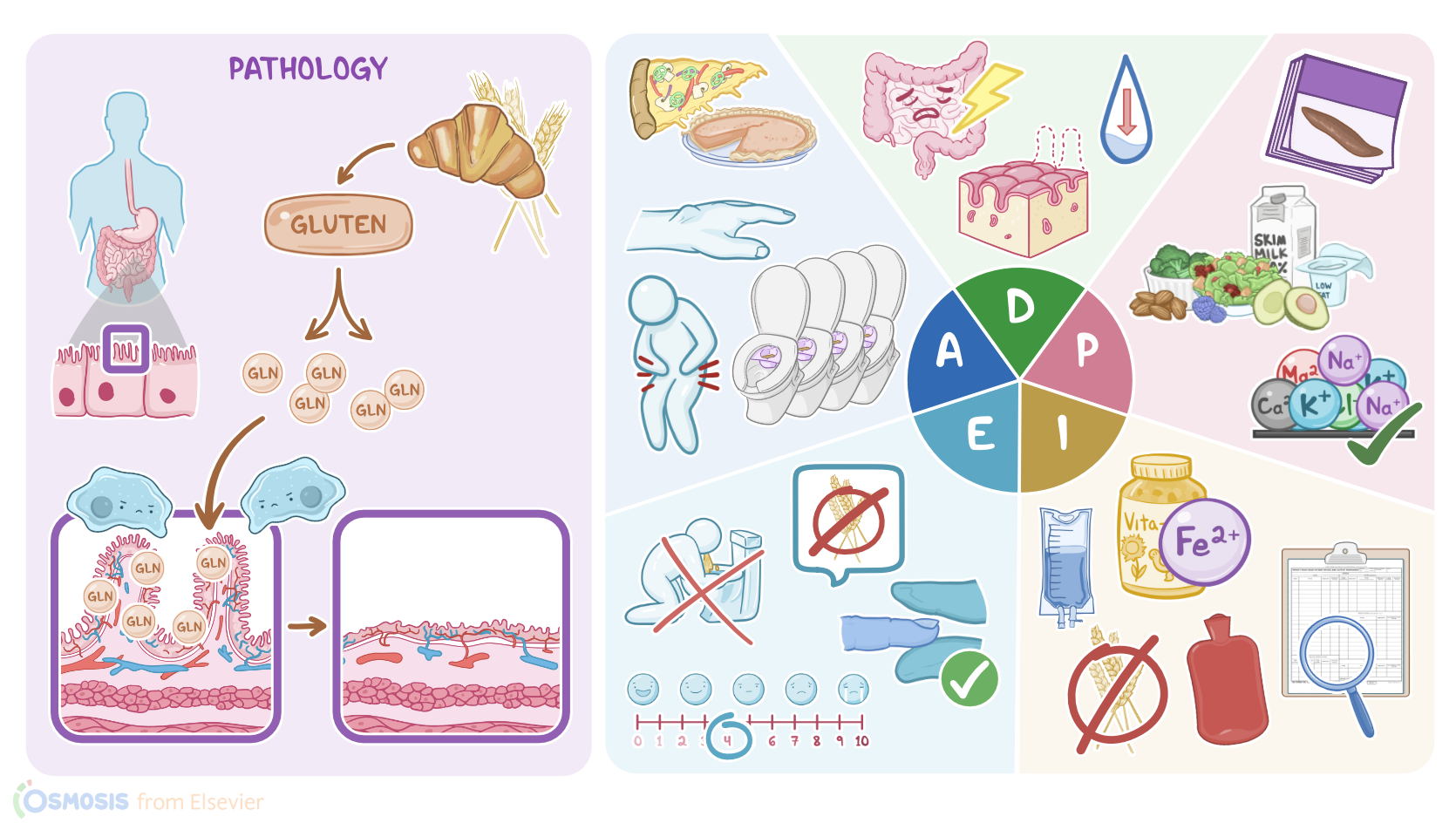
Celiac disease, also known as gluten enteropathy or celiac sprue, is currently understood as an immune-mediated disorder where the gluten in food triggers the body’s immune cells to attack the cells in the small intestine. Celiac disease is hereditary, and people with a first-degree relative with celiac disease, like a parent or sibling, have a 1 in 10 risk of developing it. Some people may be genetically predisposed to Celiac disease. In fact, it is estimated to affect 1 in 100 people worldwide.
Now, gluten’s found in all sorts of wheats and grains, including rye and barley, and is the main culprit in Celiac disease. The intestine’s inability to fully digest the protein fractions of gluten leads to a build-up of the amino acid glutamine. This accumulation is toxic to the intestinal mucosa, damaging the intestinal villi, which are those small finger-like projections that line the small intestine and help promote nutrient absorption. When the villi become damaged, they can atrophy. This leads to complications like diarrhea, vomiting, fatty stools, abdominal distention, and malabsorption of important nutrients like iron and vitamin B12-- which can lead to anemia.
Symptoms of Celiac disease are commonly first noticed between the ages of 1 and 5. Usually, there’s a period of time anywhere between 3- 6 months from the time gluten is introduced in the diet and the manifestations of Celiac disease are apparent. And of course, because gluten intake leads to complications, lifelong dietary changes are necessary in order to prevent flare-ups. Occasionally a client like Ms. Wilberson can experience an acute episode where symptoms of Celiac disease are exacerbated. This is called a Celiac crisis. The severe loss of GI contents through diarrhea and vomiting can cause complications like electrolyte imbalances, severe dehydration, and metabolic acidosis. People living with Celiac disease have a greater risk for developing coronary artery disease and small bowel cancers. And left untreated, Celiac disease can increase the chance of developing other autoimmune disorders, like Type I diabetes mellitus and multiple sclerosis.
Now that we’ve gone over the pathology, let’s look at how the nursing process can be applied. The process consists of Assessment, Diagnosis, Planning, Implementation, and Evaluation; also known as ADPIE.
So, after you greet Ms. Wilberson and introduce yourself as her nurse, you begin your assessment by first asking her how she’s feeling today. She tells you that her stomach hurts really bad and she’s feeling bloated. She then continues on to express that she has no appetite, and thinks she “overdid it with the food” at her company party a night ago, sharing that she had lots of pastries, breaded chicken tenders, and pizza, and expresses that she understands she made improper food choices. She states that she’s had several loose stools since she was admitted, last using the bathroom just before you entered, and has vomited “only a few times last night”. You check the bathroom and observe that there’s a toilet hat in place with stool present; foul-smelling and fatty in appearance. You ask Ms. Wilberson how many bowel movements she’s had since admission and she reports “4 or 5”. As you listen to Ms. Wilberson describe her symptoms, you’re visually assessing her and notice that her arms and legs appear very thin. Her lips and mucous membranes are dry. Upon closer inspection of her abdomen, you observe its distended and auscultate hyperactive bowel sounds. You assess her capillary refill and skin turgor and notice both are decreased. Ms. Wilberson’s vital signs are HR 117, RR: 20 BP: 108/70, Oral Temp.: 99.9° F, Pain: 7/10. Next, you review her recent lab results, and note the following: BUN level of 22 mg/dL, sodium level of 150 mEq/L, hemoglobin 11 g/dL, hematocrit 33%, RBC 3.8 cells/mcL, MCH 22.3 pg, MCHC 32.2 g/dL, MCV is 75 fL, RDW 18.1%. Finally, you document all your assessment findings before leaving the room.
Now after you’ve completed your assessment, you prepare a few nursing diagnoses, or clinical judgments about Ms. Wilberson’s responses to her health problem, Celiac disease. These diagnoses help nurses determine what to anticipate, or watch out for, in your clients. In doing so, you can think ahead and make a plan to address these issues! Based off the assessment data you’ve collected, your diagnoses include: acute pain related to intestinal inflammation, readiness for enhanced knowledge related to dietary restrictions, Diarrhea related to malabsorption secondary to celiac disease, dehydration related to excessive gastric loses, electrolyte imbalance related to increased gastrointestinal loses, and anemia related to malabsorption secondary to celiac disease.
As you begin planning Ms. Wilberson’s care you’re sure to keep in mind prioritizing her most important needs first. Well, now that you’ve gathered lots of information and have formed some great nursing diagnoses, it’s time to actively collaborate with other members of the interdisciplinary team to provide and develop a holistic plan of care to help Ms. Wilberson achieve the goals and desired outcomes to restore her overall well-being. Reflecting on the assessment data you’ve collected and the nursing diagnoses you’ve created, you determine the prioritization of goals include restoration of normal bowel habits by discharge; adequate fluid volume status by discharge, her electrolyte values will be within normal limits by discharge, she’ll adopt adequate daily intake of dietary iron by discharge, she’ll be pain-free by the end of shift, and understanding and commit to life-long dietary modifications by discharge.
After collaborating with the team and obtaining the necessary orders, you review the plan of care with the nursing assistant assigned to help Ms. Wilberson with her basic care needs, so you delegate the collection of I&Os. Collecting this information is important to monitor Ms. Wilberson’s diarrhea and to determine her fluid volume status. Ms. Wilberson is receiving IV fluids as well, so you remind the nursing assistant to alert you if the fluid bag running low. In the meantime, you’ll focus on assessing skin turgor and mucous membranes to determine if fluid balance restoration has been effective then follow up to ensure the physician’s order for labs has been inputted so you can continue to monitor her lab results.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "The Gluten-Free Diet for Celiac Disease and Beyond" Nutrients (2021)
- "Celiac disease: a comprehensive current review" BMC Med (2019)
- "Harrison’s Principles of Internal Medicine. 21st edition" McGraw Hill / Medical (2022)
- "Celiac Disease: Fallacies and Facts" Am J Gastroenterol (2021)
- "Updates in the diagnosis and management of coeliac disease" Best Pract Res Clin Gastroenterol (2023)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)