Myocardial infarction (MI): Nursing process (ADPIE)
2,319views
Myocardial infarction (MI): Nursing process (ADPIE)
Acute Final
Acute Final
Notes
| MYOCARDIAL INFARCTION (MI) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
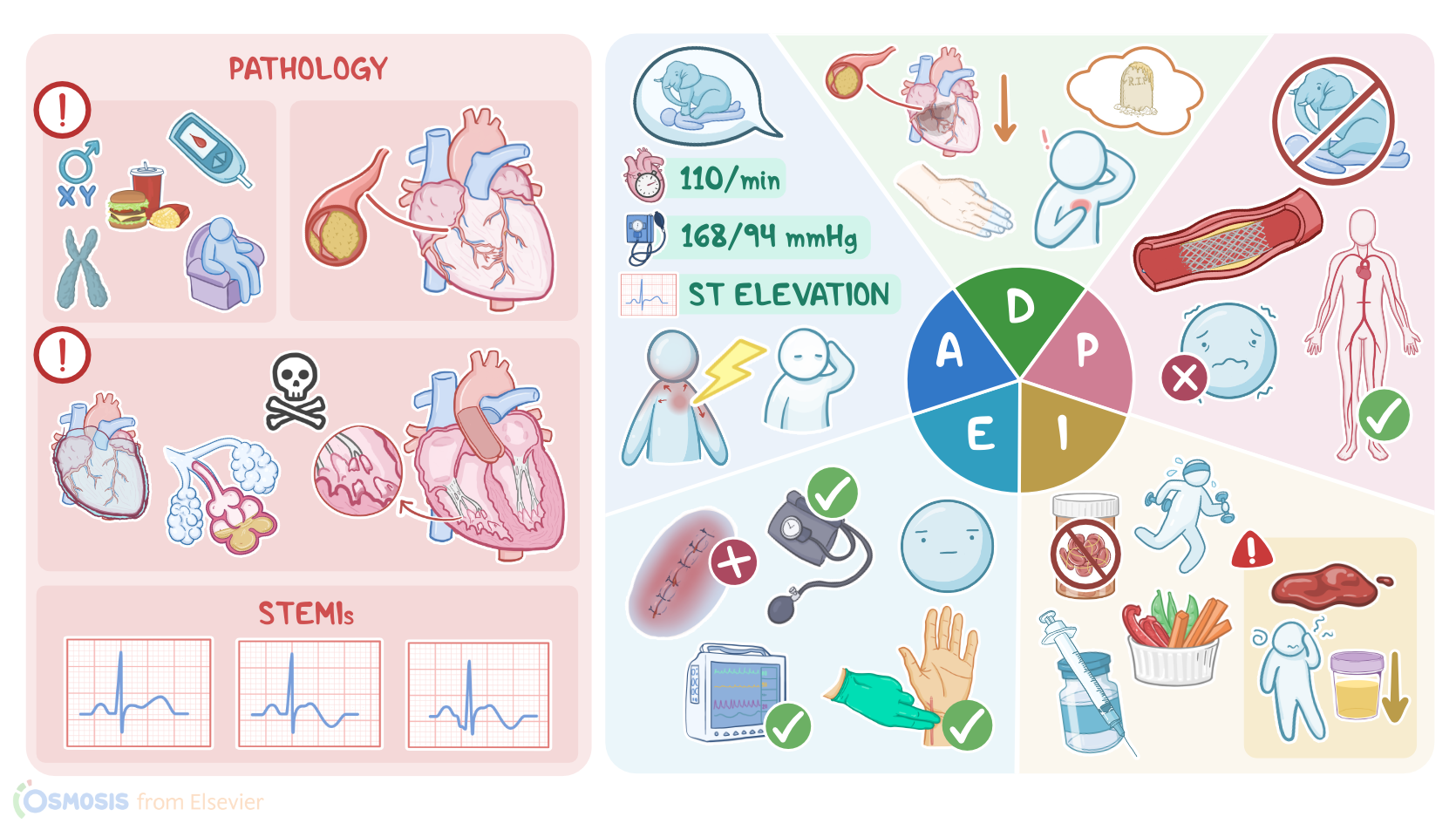
Miguel Garcia is a 60-year-old Hispanic male with a history of hypertension who was brought to the emergency department, or ED, for chest pain.
The pain began two hours ago and he states it feels like an elephant is sitting on his chest.
The physician just confirmed with an electrocardiogram, or ECG, that Mr. Garcia is experiencing a STEMI, which stands for ST segment elevation myocardial infarction.
The team is acting swiftly to prepare him for an emergent percutaneous coronary intervention, known as a PCI.
A myocardial infarction, also known as an MI or heart attack, refers to the death of cardiac muscle tissue from prolonged ischemia.
Risk factors include being over 40 years old or male; having diabetes mellitus, dyslipidemia, hypertension, or a family history of MIs; smoking tobacco; obesity; a sedentary lifestyle; and eating a high fat diet.
The most common cause of MI is atherosclerosis. This is when lipid containing plaque builds up in the coronary arteries.
When the coronary artery is occluded, blood and oxygen supply cannot meet the demands of the myocardium, causing ischemia.
This leads to angina, or a type of chest pain. Angina can either be stable or unstable.
Stable angina is provoked by activities that increase oxygen demand, such as exercise, lasts up to 15 minutes, and is relieved by rest or vasodilators like nitroglycerin.
This is because the occlusion limits blood flow while the oxygen demand of the myocardium increases, but when demand decreases or if the artery becomes dilated, the pain resolves
On the other hand, unstable angina can occur without exertion or even at rest, persists longer than 15 minutes, is a more severe pain than stable angina, and is not relieved by rest or vasodilators.
This is often due to the plaque rupturing which causes platelets to attach to the plaque, forming a thrombus.
The result is a more severe reduction in coronary blood flow than what occurs in stable angina, so it doesn’t resolve with rest or vasodilators.
Initially, ischemic damage is potentially reversible, but after about 20 to 40 minutes the damage is irreversible and myocardial tissue starts to necrose, causing an MI.
During an MI, the lack of blood supply to the myocardium can cause severe crushing substernal chest pain.
The pain is unprovoked, which means it occurs spontaneously regardless of activity, persists over thirty minutes, is unrelieved by rest or vasodilators like nitroglycerin, and can radiate to the shoulders, arms, jaw, neck, or back.
The myocardial oxygen supply and demand imbalance during an MI can also lead to blood pressure and heart rate changes, dysrhythmias, dyspnea, nausea, vomiting, fever, diaphoresis, a feeling of impending doom, and coolness or cyanosis of the extremities.
However, symptoms can vary greatly.
Women and elderly clients are more likely to experience atypical symptoms, and about 20 percent of MIs are silent, meaning the client was asymptomatic or attributed symptoms to another condition, such as heartburn.
The damage caused to the myocardium during an MI can lead to several complications, including arrhythmias, cardiogenic shock, pericarditis, heart failure, papillary muscle rupture, pulmonary edema, and sudden cardiac death.
If an MI is suspected based on symptoms, the next step is to diagnose it as soon as possible.
When it comes to diagnosing MIs, there are two types to keep in mind based on the ECG findings: NSTEMIs, or non ST segment elevation myocardial infarction, and STEMIs.
During an MI, the inner third of the myocardium, called the subendocardium, is affected first because it’s farthest from the coronary arteries making it more vulnerable to changes in coronary perfusion.
If the infarct is limited to the subendocardium, this is known as a subendocardial infarction and shows on an ECG with a depressed or non-elevated ST segment.
If the necrosis spreads beyond the endocardium, it’s called a transmural infarction and will have ST segment elevation on an ECG.
Other ECG findings may include the presence of inverted T waves and new Q waves during a STEMI, and T wave inversion during an NSTEMI.
For a client with unstable angina, the ECG findings are typically normal.
A clear way to differentiate between angina and a MI is with cardiac biomarkers.
Cardiac biomarkers are only present in the case of a MI because they indicate there has been irreversible damage to the myocardium.
These include troponin I, troponin T, and creatinine kinase isoenzyme MB, called CK-MB.
Troponin I and T, which are specific markers of cardiac injury, are elevated 2 to 4 hours after an infarction, peak around 48 hours, and remain elevated for 7 to 10 days.
CK-MB levels also start to rise 2 to 4 hours after an infarction, peak around 24 hours, and remain elevated for 48 hours.
Although CK-MB is not specific to cardiac injury, it is useful for identifying a reinfarction before troponin levels have returned to normal.
Because cardiac biomarkers can take several hours to be detected, they should be checked initially upon client arrival and again 6 hours later.
Now, treatment should be initiated as soon as possible when a STEMI is diagnosed to restore perfusion to the myocardium.
Oxygen should be administered to clients who are breathless, have an oxygen saturation less than 90 percent, or who have heart failure.
Chewable aspirin should be administered to slow clotting.
Vasodilators, like nitroglycerin, should be administered to foster coronary vasodilation but are contraindicated in clients with hypotension, bradycardia, or who have taken phosphodiesterase inhibitors in the past 72 hours.
Pain control increases myocardial oxygenation, so an analgesic such as morphine should be administered too.
Within 30 minutes of client arrival, a chest x-ray should be performed to detect cardiomegaly, pulmonary edema, pleural effusion, aortic dissection, or heart failure.
A complete blood count should be performed to assess for anemia and to obtain a baseline platelet count prior to initiating thrombolytic therapy.
A complete metabolic panel can reveal abnormalities in electrolytes and kidney function.
Also, clotting times may be ordered to establish baseline levels for anticoagulation therapy.
Once a STEMI is confirmed, reperfusion is needed immediately and can be accomplished through PCI; thrombolytic therapy, also called fibrinolytic therapy; or a coronary artery bypass graft, referred to as CABG.
Emergent PCI is the preferred reperfusion strategy and should be performed within 90 minutes of client arrival to the ED.
PCI involves inserting a catheter into the femoral or radial artery, injecting contrast to locate the occlusion, inflating a tiny balloon to compress the obstructing plaque, and inserting a stent to keep the artery patent.
If PCI is unavailable, thrombolytic therapy should be administered within 30 minutes of client arrival to the ED.
Thrombolytic therapy involves IV administration of a thrombolytic medication, such as reteplase, to dissolve the occluding clot.
CABG, which involves grafting a vein or artery from elsewhere in the body onto the coronary artery to bypass the blockage.
It’s not used as frequently as PCI or thrombolytic therapy but is indicated when PCI is unsuccessful.
If more than 12 hours have passed since symptom onset, reperfusion strategies are generally not performed, but PCI may be considered for clients with ongoing ischemia.
After reperfusion or if reperfusion couldn’t be done, anticoagulation agents, such as heparin, are administered, in addition to dual antiplatelet therapy using aspirin and a PY12 inhibitor like clopidogrel.
Cardioprotective medications, including angiotensin converting enzyme, or ACE inhibitors; angiotensin receptor blockers, or ARBs, for clients intolerant of ACE inhibitors; beta blockers; and statins are recommended as long term therapy after a STEMI.
Additionally, lifestyle modifications, like following a low fat and low salt diet, exercising, and smoking cessation, as well as enrolling in a cardiac rehabilitation program are important aspects of post STEMI care.
All right, let’s get back to Mr. Garcia and begin his assessment.
Upon entering his exam room, you introduce yourself, confirm his identity, and perform hand hygiene.