Physical assessment - Neonate: Nursing
Physical assessment - Neonate: Nursing
Watch later
Watch later
Notes
| PHYSICAL ASSESSMENT - NEONATE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
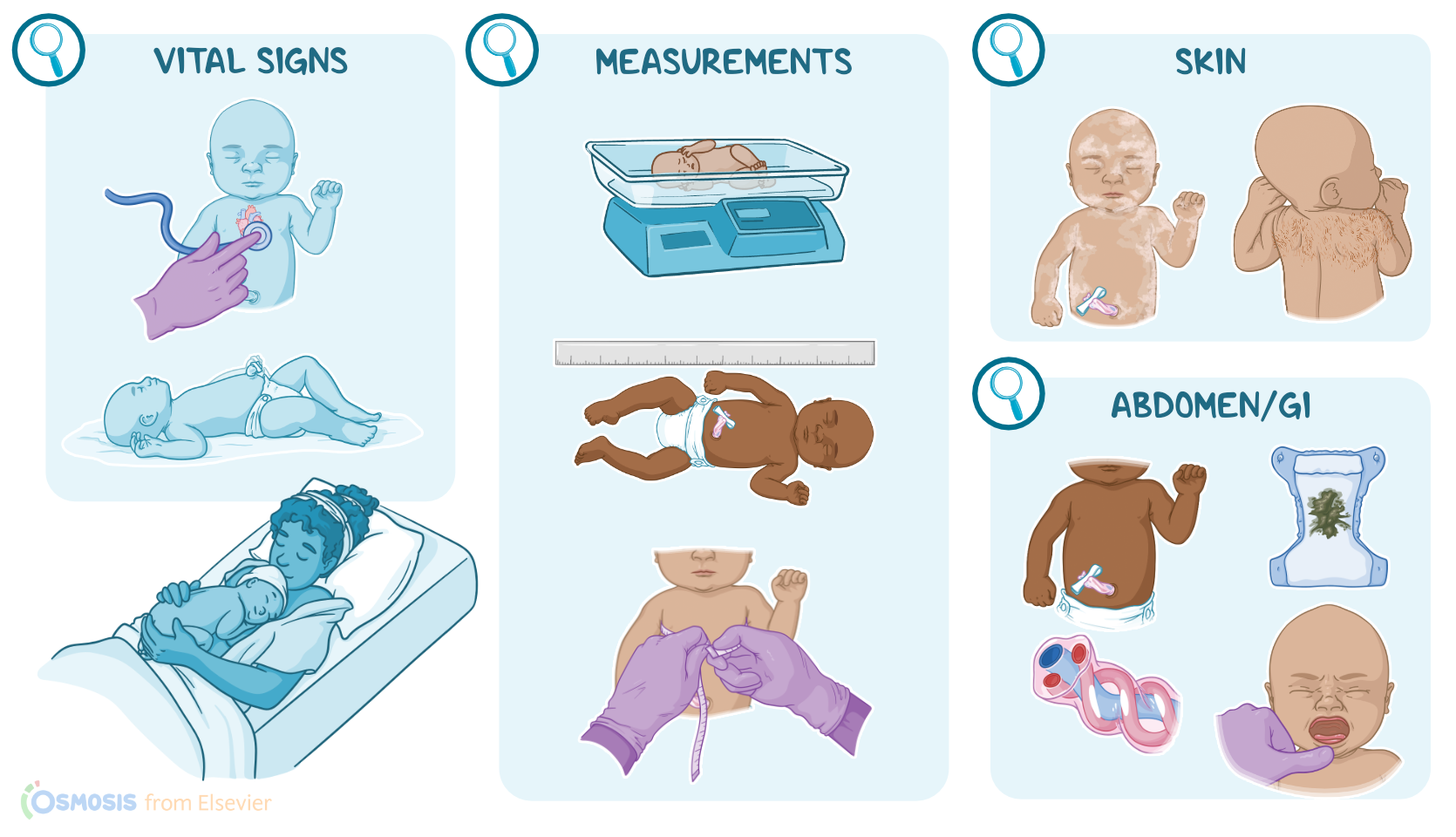
| VITAL SIGNS |
| |
| MEASUREMENTS |
| |
| SKIN |
| |
| HEAD |
| |
| EYES AND EARS |
| |
| CARDIOVASCULAR |
| |
| CHEST AND LUNGS |
| |
| ABDOMEN AND GI SYSTEM |
| |
| GENITOURINARY |
| |
| MUSCULOSKELETAL |
| |
Transcript
The physical assessment of a newborn is an ongoing process to monitor the newborn’s adaptation to extrauterine life, and to identify problems that need immediate intervention. At the same time, the assessment considers factors such as the prenatal history; any complications during the pregnancy, labor, and birth; the type of anesthesia or analgesia used during birth; if any neonatal resuscitation measures were needed; and the newborn’s gestational age.
Let’s start by looking at the newborn’s vital signs. First, the apical pulse is auscultated. It’s a good idea to assess this first, when the infant is in a quiet state, and before any other assessments which could agitate them. A newborn’s heart rate normally varies between 120 and 160 beats per minute, but it can rise to 180 beats per minute when the infant is crying or drop as low as 80 to 90 beats per minute when in deep sleep. A consistently high or low heart rate should be investigated.
Next up is the newborn’s respirations. Respirations are usually irregular, and there may be occasional 5 to 20 second pauses; so they are counted for a full minute for accuracy. A normal respiratory rate is between 30 to 60 breaths per minute. You’ll notice that the abdomen will rise and fall with each respiration; this is normal, because newborns tend to use their diaphragm to breathe more than their intercostal muscles. A respiratory rate of more than 60 breaths per minute could signal problems like cold stress, congenital heart defects, or infection; while a respiratory rate less than 30 breaths per minute could be associated with central nervous system depression.
Then, the temperature is measured, which normally ranges between 97.7° F and 99.5° F, or 36.5° C and 37.5° C. The axillary temperature is the preferred method of measurement, because it is easily accessed and is a close estimate to the newborn’s core temperature
Blood pressure is not routinely measured in well newborns, except when there are murmurs or other signs of cardiac complications, in which case it is measured on both the upper and lower extremities. Normal newborn blood pressure ranges between 60 to 80 mmHg systolic over 40 to 50 mmHg diastolic.
The next step in newborn assessment is to determine their measurements, including the weight, length, head, and chest measurements. These are compared to the normal values for the infant’s gestational age. Normal weight for term newborns ranges between 2500 grams to 4000 grams. The length of the infant is measured from the top of the head to the heel of the outstretched leg and ranges between 48 to 53 centimeters or 19 to 21 inches. Next, the head circumference is measured around the occiput, or back of the head, and above the eyebrows. Normal values are between 33 to 35.5 centimeters or 13 to 14 inches, but that can be affected when the cranial bones overlap as the head is squeezed during birth, in a process called molding. The chest is measured at the nipple line and is usually about 2 to 3 centimeters smaller than the head, with a normal range of 30.5 to 33 centimeters or 12 to 13 inches.
Next, let’s look at the neonate’s skin. First, vernix caseosa, which is a creamy white substance that protects the fetal and newborn skin, may cover the entire body, or it may be concentrated between skin folds. A fine, downy hair called lanugo will also be seen, especially on the back between the shoulders.
The newborn's skin should be soft, smooth, and opaque, and there can be some variations from the normal range of skin coloration. Acrocyanosis, meaning bluish discoloration of the hands and soles of the feet, is normal during the first few hours of life, and is thought to be caused by vasomotor instability during transition from fetal to neonatal life. It normally resolves within 24-48 hours, but could be aggravated if the infant is cold. Another common type of cyanosis is bluish discoloration around the mouth, referred to as circumoral cyanosis, which can last up to 24 hours.
Color changes that should be investigated include circumoral cyanosis that persists more than 24 hours; acrocyanosis that lasts longer than 48 hours; jaundice or yellowing of the skin or sclera, especially if it appears within the first 24 hours of life; plethora, which is a ruddy skin tone that could signal an excess of RBCs, or polycythemia, and an unusually high hematocrit, commonly associated with maternal smoking, diabetes, or preeclampsia; pallor, or paleness can be an indication of poor perfusion; and lastly, central cyanosis, cyanosis that does not improve with supplemental oxygen, or cyanosis that appears when the infant is crying could be associated with a congenital heart defect or infection.
Now, there are some transient skin changes that are normal in newborns. First, there’s erythema toxicum, which sounds bad, but it’s a benign reddish-pink rash with yellowish-white papules that can be seen on the face, chest, and extremities. The rash is also referred to as simply “newborn rash” and it usually resolves spontaneously within 4 to 5 days. Most newborns also have small pearly white papules, about the size of a pinhead, scattered across the brow, nose, chin, and cheeks. These are called milia, and they are caused by a buildup of sebaceous gland secretions. Milia usually disappear within a few weeks.
Finally, there are some common birthmarks to note during your assessment. You may notice pale pink spots commonly found on the nape of the neck, eyelids, or forehead in newborns with light skin. These are called nevus simplex, and are sometimes referred to as “stork bite” or “angel kiss”, and they usually fade by the second year of life. Then there’s dermal melanocytosis, which are large bluish-gray macules that are commonly found on the sacrum, buttocks, and shoulders in newborns of color. These usually fade gradually over the first 2 years of life.
Okay, moving on to the newborn’s head. Gently palpate the fontanelles, or “soft spots” which are openings in the spaces at the intersections of the sutures. The main fontanelles are the anterior and posterior one, and both should be flat and soft. The diamond-shaped anterior fontanel is 4 to 6 cm at birth, and closes between 18 and 24 months. The triangular posterior fontanelle is less than 0.5 cm at birth, and it will close by 2 to 3 months of age. You may notice that the anterior fontanelle pulsates with the heartbeat or may swell during crying, but a bulging, tense fontanelle is a sign of increased intracranial pressure.
Next, check the head for evidence of birth trauma. Often you’ll notice some swelling on the head. If the swelling is soft, boggy, with irregular margins that override the suture lines, then this is scalp edema referred to as a caput succedaneum or caput for short. It’s caused by pressure on the head during birth, which compresses blood vessels in the scalp, causing fluid to leak between the scalp and the periosteum of the skull. A caput will be present at birth, and it usually resolves within a few days.
On the other hand, a collection of blood between the periosteum and the skull is called a cephalohematoma. It’s also caused by pressure on the skull, but unlike a caput, there’s a shearing pressure that occurs in a deeper and more vascular part of the fetal skull. It may not be present immediately after birth, but will slowly develop over the next several hours, and take several weeks to resolve. Also unlike a caput, the edges of a cephalohematoma will be clearly defined, since the bleeding is contained by the suture lines. Newborns with a cephalohematoma should be watched closely for hyperbilirubinemia, since the extra RBCs in the hematoma will be slowly destroyed, creating an increase in unconjugated bilirubin.