Smoke inhalation injury: Nursing process (ADPIE)
Smoke inhalation injury: Nursing process (ADPIE)
223 Content
223 Content
Notes
| SMOKE INHALATION INJURY | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Janine Jones is a 35-year-old female who was brought to the emergency department, or ED, by ambulance after being trapped in her home during a fire.
Firefighters responded when a neighbor noticed smoke coming from Janine’s home.
Janine appears alert and oriented but she is unsure how long she was stuck in her home.
She presents with coughing, shortness of breath, and a hoarse voice.
She is admitted to the intensive care unit or ICU, with smoke inhalation injury.
Smoke inhalation injuries occur when the airways or lungs are damaged from inhaling heat, irritant particulates, or toxic chemicals present in smoke.
The most common scenario involves being in a house fire or other enclosed space during a fire.
Now, there are some factors that may put an individual at risk for an inhalation injury during a fire.
Non-modifiable risks include age, in particular young children and the elderly, as well as those with physical or mental disabilities.
These factors can make it harder for the individual to stop a fire, or escape from it.
In addition, having an underlying lung disorder increases the risk of harm from smoke inhalation.
On the other hand, modifiable risk factors include being in a building without functioning smoke detectors, or being under the influence of alcohol or drugs during a fire.
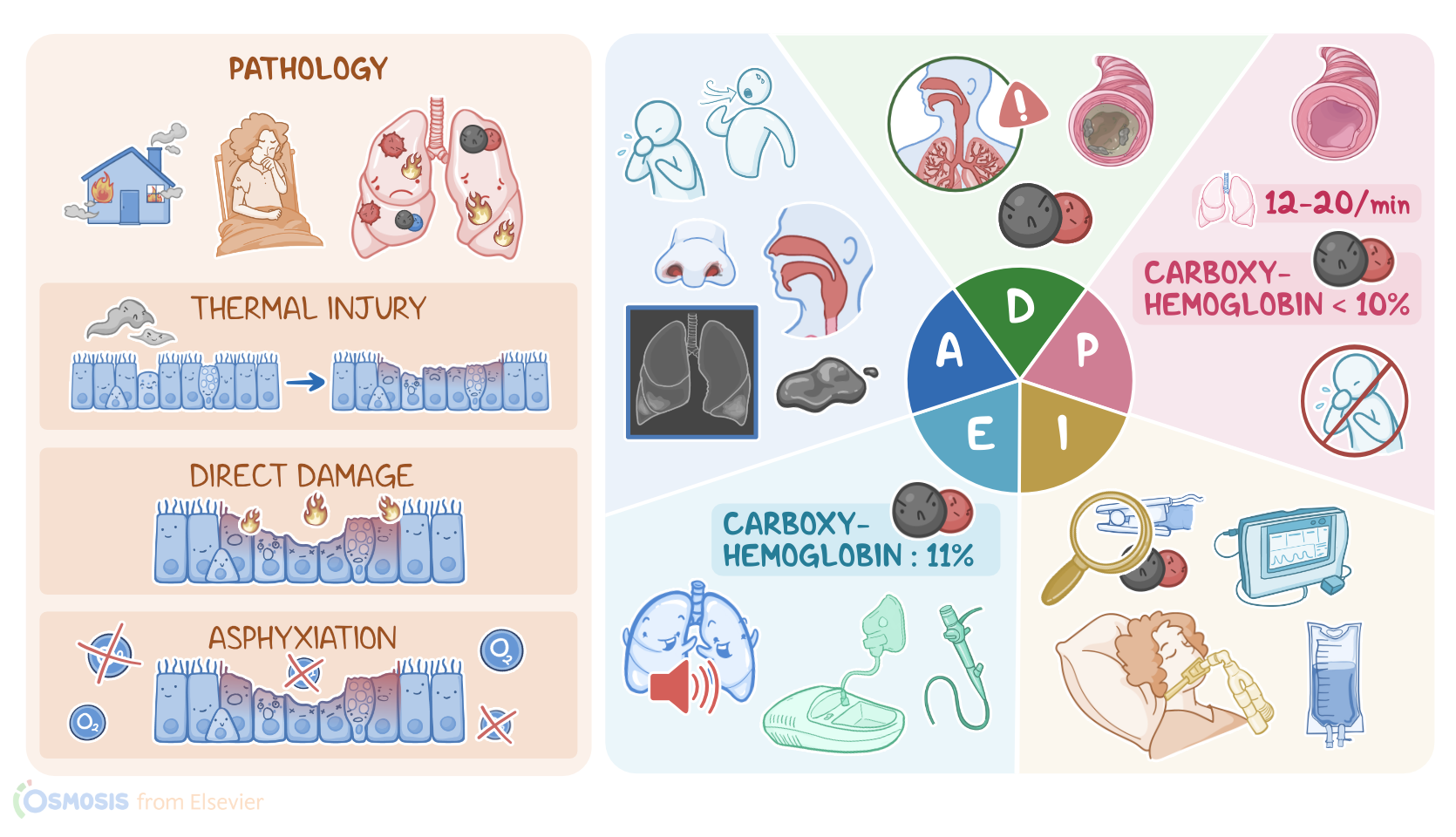
Now, once the smoke is inhaled into the airways, it can cause three main types of airway injury.
The first type is thermal injury, which is when the heat from the smoke burns the epithelium lining the airway.
The second type of injury comes from particulates and chemicals that can irritate and cause direct damage to the airway.
And third, smoke inhalation can cause asphyxiation, where oxygen availability and use by the tissues is impaired.
The signs and symptoms associated with a smoke inhalation injury typically depend on the duration and extent of exposure, and how far the inhaled smoke travels down the airways.
First there’s upper airway injury, which involves direct thermal damage from heat to the mouth, oropharynx, and larynx.
This mainly leads to local erythema, as well as ulceration and sloughing of the airway epithelium.
Other frequent signs of upper airway injury include a hoarse voice due to vocal cord damage, and dark grey or black sputum, referred to as carbonaceous sputum.
In addition, some clients may develop localized edema.
If the edema becomes severe enough, it can obstruct the airway, leading to dyspnea and stridor, which is a harsh, grating sound when breathing.
If the smoke makes its way a bit further down the airway, the particulates and chemicals that are directly toxic to the tracheobronchial epithelium and can result in bronchospasm, a productive cough associated with bronchorrhea or excessive mucus discharge, as well as wheezing, which is a high-pitched whistling sound that usually happens during exhalation.
Particulates and chemicals that are small enough to travel all the way down to the lungs, can cause damage to the bronchioles and alveoli.
Initially, parenchymal injury doesn’t show any symptoms, but within a few hours, an inflammatory response results in edema and increased pulmonary capillary permeability.
The client might develop atelectasis, which is when the part of the lung collapses, resulting in dyspnea and decreased breath sounds, tachypnea, the use of accessory respiratory muscles, and systemic hypoxia.
Clients experiencing smoke inhalation injury often develop complications.
One of the main complications is systemic toxicity from the products of combustion, including carbon monoxide and cyanide.
Pneumonia is a common complication, since microbes can more easily access and invade the damaged respiratory tract.
Pulmonary edema can be the result of lung inflammation.
Another important complication is acute respiratory distress syndrome, or ARDS, which is when fluid builds up in the alveoli, impairing their ability to get enough oxygen into the blood.
Ultimately, this can lead to respiratory failure, resulting in severe tissue hypoxia, as well as end-organ damage, and death.
Fortunately, most clients who survive a smoke inhalation injury don’t develop long term complications.
However, some important ones to keep in mind include permanent tissue damage, such as tracheal stenosis or scarring that leads to airway narrowing; bronchiectasis with damaged and thickened bronchi; bronchiolitis obliterans, which is characterized by extensive scarring and obstruction of the bronchioles; and interstitial fibrosis with scarring of the lung tissue.
The main diagnostic studies used in the case of an inhalation injury include standard laboratory tests, such as a complete blood count, which often reveals an increased neutrophil count, indicating inflammation and infection; decreased electrolytes like sodium and potassium; elevated blood urea nitrogen and creatinine; and elevated serum lactate levels.
In addition, blood gas analysis often shows an increased PaCO2 and decreased PaO2, and it may reveal an elevated carboxyhemoglobin indicating carbon monoxide poisoning.
Then, chest X-rays are typically done to visualize the lungs, and look for pulmonary edema.
Finally, a bronchoscopy is performed to directly examine the upper airways and bronchi for damage.
Treatment of inhalation injury is typically supportive.
The main goal is to maintain an open airway.
Clients that present with an obstructed airway, signs of respiratory distress, abnormal mental status, or severe burns to the face and neck, should be intubated immediately and ventilated mechanically.
Some clients may need a tracheostomy, which is an incision in the trachea to bypass the airway obstruction.
On the other hand, those who are not intubated early must be closely monitored, as they may rapidly develop airway edema.
All clients should receive humidified oxygen.
In addition, treatment should aim at reducing pulmonary secretions and clearing the airways from excessive mucus or epithelial sloughing.
Key Takeaways
Smoke inhalation injury is a serious medical condition that occurs when the airways or lungs are damaged from inhaling heat, irritant particulates, or toxic chemicals present in smoke during a fire. Symptoms include breathing difficulties, coughing, wheezing, and other respiratory symptoms. The severity of the injury depends on the duration and intensity of the exposure, as well as the type of materials burned.
In addition to respiratory symptoms, smoke inhalation injury can also cause systemic effects, such as carbon monoxide poisoning and chemical toxicity from other toxic gasses, which can lead to organ damage, altered mental status, and even death. Treatment for smoke inhalation injury typically involves securing the airway, administering oxygen, removing any residual smoke or debris from the airway, administering IV fluids and other supportive care as needed.