Thrombocytopenia: Nursing
1,757views
Thrombocytopenia: Nursing
Medical Surgical
Medical Surgical
Notes
| THROMBOCYTOPENIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
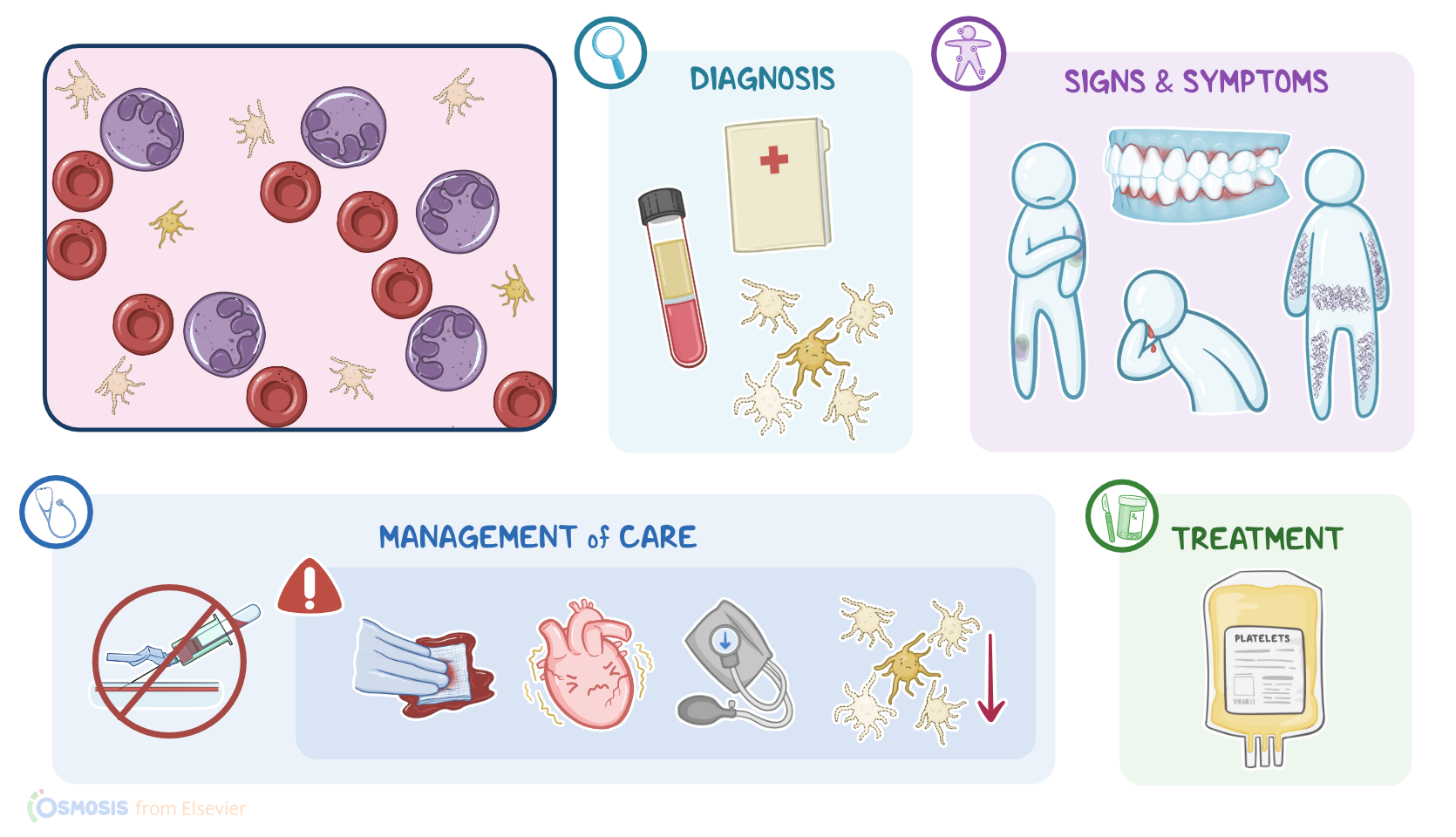
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Thrombocytopenia is when there’s a low number of platelets, also known as thrombocytes, in the blood. Normally, there are between 150,000 and 450,000 thrombocytes per microliter of blood; while in thrombocytopenia, this number goes below 150,000 cells per microliter. Remember that platelets are involved in blood clotting, so with thrombocytopenia, clients have an increased risk of bleeding.
But let’s start with some basic physiology of platelets, which form in the bone marrow. Although often called cells, platelets are actually small fragments of megakaryocytes, which themselves derive from hematopoietic stem cells, that give rise to all types of blood cells. After they’re formed, platelets leave the bone marrow to enter the bloodstream, and almost 50% of them are stored in the spleen, while the remaining keep circulating through the vascular system.
Now, when there’s any kind of damage to a blood vessel, circulating platelets aggregate to form a platelet plug at the site of the injury. This process is also known as primary hemostasis, and it’s followed by secondary hemostasis. During secondary hemostasis, clotting factors come into play one after another, eventually cleaving the fibrinogen into fibrin, which forms a protein mesh. This protein mesh is like a giant net that wraps around the platelet plug and reinforces it, stopping the bleeding.
Now, based on the cause, thrombocytopenia can be subdivided into three main groups. The first group covers conditions associated with impaired platelet production, such as inherited thrombocytopenia; viral infections, like HIV and HCV infections; folate and vitamin B12 deficiencies; and aplastic anemia. Aplastic anemia is typically associated with bone marrow suppression, and it’s characterized by decreased production of platelets as well as red and white blood cells.
The second group covers thrombocytopenias caused by increased platelet destruction or consumption, which are further subdivided into non-immune and immune-mediated. Non-immune thrombocytopenias include thrombotic thrombocytopenic purpura or TTP, hemolytic-uremic syndrome, or HUS for short, and disseminated intravascular coagulation, or DIC. Moreover, these thrombocytopenias occur because of increased consumption of platelets during the formation of abnormal clots. As a result, there are fewer platelets left in circulation.
On the flip side, immune-mediated thrombocytopenias include heparin-induced thrombocytopenia, or HIT, and immune thrombocytopenic purpura, or ITP. In immune-mediated thrombocytopenia, the body produces antibodies that bind platelets and induce their destruction.
Finally, the third group covers conditions associated with the impaired distribution of platelets, such as hypersplenism and massive blood transfusion. Hypersplenism typically occurs when there’s liver cirrhosis and portal hypertension. As a result, the blood backs up into the spleen, which allows up to 90 percent of the total platelets in. This means that nearly no platelets are left in the blood.
On the flip side, with massive blood transfusions, the platelet concentration falls as a result of large volume transfusions of platelet-free products, like packed red blood cells or intravenous fluids. The mechanism behind thrombocytopenia associated with blood transfusion is actually hemodilution, meaning the same amount of platelets now circulate in a much larger circulating volume.
Now, important risk factors for developing thrombocytopenia include autoimmune conditions, like systemic lupus and rheumatoid arthritis; infections with some strains of E. coli that can cause HUS; and cancers, such as leukemia and lymphoma. Other important risk factors include alcohol; the use of medications, like aspirin and heparin.
Now, pathology-wise, with thrombocytopenia, it’s more difficult to form a platelet plug at the site of injury, so there’s an increased risk of bleeding. Moreover, once bleeding occurs, it takes more time to stop.
Thrombocytopenia can also cause life-threatening complications if not recognized on time. For example, when platelet count falls below 20,000/microliter a client might experience spontaneous bleeds, and if their platelet count falls below 10,000/microliter they can even develop spontaneous intracranial bleeding.
Additionally, in clients with thrombotic thrombocytopenic purpura, platelets tend to aggregate excessively at abnormal sites, so where there isn’t any reason. This can cause microthrombi and, as a consequence, thrombosis-related complications, such as deep vein thrombosis, pulmonary embolism, organ infarctions, or even stroke.
Now let’s translate this into a clinical picture. One of the first clinical manifestations of thrombocytopenia is bruising easily after minor trauma. Other important clinical manifestations include mucosal bleeding, like gingival bleeding or nosebleeds; and cutaneous bleeding, which can manifest as petechiae, or pinpoint superficial skin bleeds; purpura, or coalesced petechiae; and finally, ecchymoses, which are even larger areas of accumulated blood.
Finally, clients with TTP are at a higher risk of thrombosis so they might have a stroke with symptoms like headaches, changes in vision, unilateral weakness or paralysis of the face, arm or leg, difficulty talking or swallowing, and confusion. They’re also at a higher risk of pulmonary embolism and have symptoms like chest pain and shortness of breath.
Diagnosis of thrombocytopenia starts with the client’s medical history and physical assessment. Additionally, a complete blood count reveals a platelet count below 150,000/microliter. Specifically, mild thrombocytopenia, when platelet count is between 100,000 and 150,000; moderate thrombocytopenia, when it’s between 50,000 and 100,000; and finally, severe thrombocytopenia when there are less than 50,000 platelets per microliter of blood.
Coagulation studies can also be done, but it’s important to remember that with thrombocytopenia, prothrombin time and partial thromboplastin time are normal. That’s because this test gives information regarding secondary hemostasis, not platelet plug formation. A peripheral blood smear usually reveals scarce platelets; while fecal occult blood testing and urinalysis can reveal blood in the stool or the urine, respectively.
Additionally a bone marrow biopsy can reveal abnormal megakaryocytes, which indicate platelet problems, or scarce amounts of all blood cells and their precursors, in aplastic anemia. Finally, with immune-mediated thrombocytopenia, an important part of diagnosis is the detection of autoimmune antibodies.
Next, treatment depends on the type of thrombocytopenia. For example, in thrombotic thrombocytopenic purpura, treatment includes plasma exchange. On the flip side, clients with heparin-induced thrombocytopenia require discontinuation of the medication and administration of a direct thrombin inhibitor, like dabigatran or argatroban.
In patients with immune thrombocytopenic purpura, the first-line treatment is glucocorticoids; while the second-line is IV immunoglobulins. If both treatments fail, these clients should undergo splenectomy or removal of the spleen. Finally, no matter what the cause is, platelet transfusion is indicated in all clients with a severe hemorrhage or platelet count below 10,000/microliter.
Key Takeaways
Thrombocytopenia is a medical condition characterized by a low platelet count in the blood. Normally, platelets are responsible for blood clotting, and a low platelet count can lead to bleeding, bruising, and other complications. Thrombocytopenia is said when platelet count falls below 150,000.
Thrombocytopenia can be caused by diseases that decrease platelet production, platelet sequestration in the spleen, or increase platelet destruction by non-immune or immune-mediated mechanisms. Diagnosis begins with a history and physical assessment, along with laboratory tests like a CBC, peripheral blood smear, and bone marrow biopsy. Treatment depends on the type of thrombocytopenia. Treatment of thrombocytopenia involves treating the underlying cause, and transfusing platelets when the platelet count is less than 10,000, or less than 50,000 if the patient is actively bleeding or about to undergo a major surgical procedure. Priority goals of nursing care for a client with thrombocytopenia include prevention and early detection of bleeding, as well as intervening when bleeding occurs. Client and family teaching focuses on lifestyle changes and safety precautions to prevent bleeding, and when to contact the healthcare provider.