Tuberculosis (TB): Nursing
1,371views
Tuberculosis (TB): Nursing
Watch later
Watch later
Notes
| TUBERCULOSIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Tuberculosis or TB for short is an infectious disease that primarily affects the respiratory tract, and is caused by Mycobacteria spp., such as Mycobacterium tuberculosis.
Now, let’s quickly review the respiratory tract, which can be divided into two regions: the upper respiratory tract and lower respiratory tract. The upper respiratory tract includes the nose, nasal cavity, the oral cavity, pharynx, epiglottis, larynx, and the upper part of the trachea; while the lower respiratory tract includes the lower part of trachea, and the lungs containing the bronchi, bronchioles, alveolar ducts, and finally the alveoli. Alveoli are tiny air-filled sacs where most gas exchange occurs, so as we breathe, the inhaled oxygen moves from the alveolar sacs into the blood, while the carbon dioxide moves from the blood into the alveolar sacs to be exhaled.
Now, TB is caused by Mycobacteria spp. settling in the bronchioles and alveoli. The majority of TB cases are caused by Mycobacterium tuberculosis. However, it can rarely be caused by Mycobacterium bovis, Mycobacterium africanum, and Mycobacterium microti. These bacteria are transmitted from person to person via respiratory droplets. This happens when a person with active TB talks, sneezes, or coughs, spreading droplets that may then be inhaled by others nearby.
Risk factors for TB include close contact with an infected individual, as well as living in crowded areas, working in a healthcare facility, having limited access to healthcare, not being vaccinated, experiencing homeless, and alcohol or IV drug abuse.
In addition, children and immunocompromised individuals are at higher risk for TB; these include clients with HIV, cancer, malnutrition, diabetes, elderly clients, or those taking immunosuppressant medications like corticosteroids.
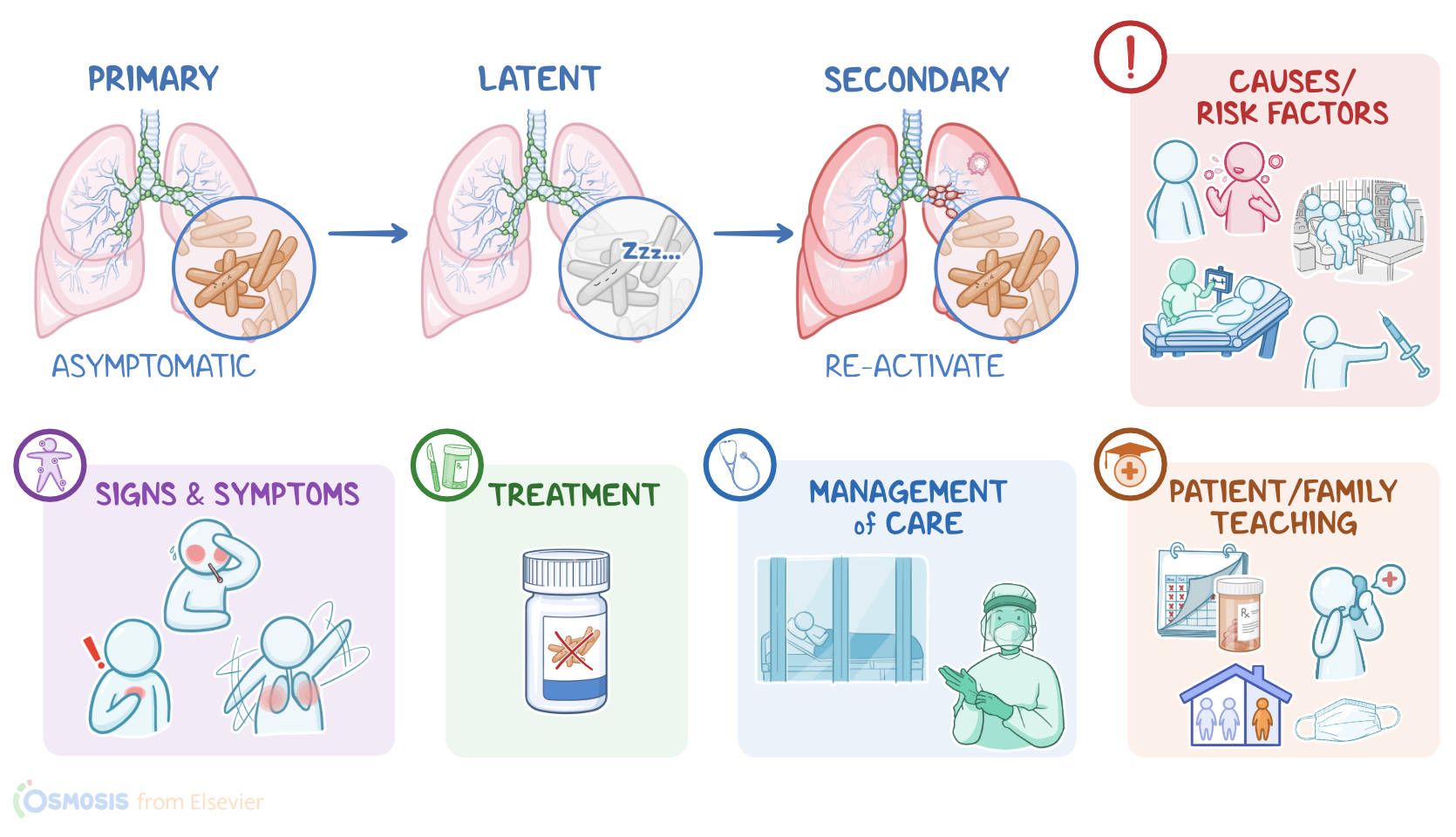
Now, there are various stages of TB infection. Primary tuberculosis occurs when an individual is exposed to mycobacteria for the first time. These bacteria can make their way to the bronchioles and alveoli. In children or immunocompromised clients, the immune system can’t contain the infection, so it spreads throughout the lungs, causing further damage and bronchopneumonia; this stage is called progressive primary tuberculosis.
On the other hand, in immunocompetent individuals, the infection activates local macrophages that eat up and destroy the mycobacteria, forming small tuberculous caseating granulomas, called Ghon lesion or focus. This leads to a stage called latent tuberculosis, where the granulomas can only contain the infection and prevent further damage, but mycobacteria are able to survive and remain dormant inside these granulomas, even for years.
Finally, if the client’s immune system becomes compromised later on, mycobacteria can become reactivated, leading to secondary tuberculosis. At this point, the infection may spread throughout the lungs, forming more Ghon lesions in addition to fibrocaseous cavities due to necrosis and destruction of lung tissue, causing bronchopneumonia. In the worst cases, the infection in both secondary and progressive primary tuberculosis can spread via the bloodstream, causing bacteremia; as a result, TB can become widespread and infect almost every other tissue in the body, leading to miliary tuberculosis.
So, TB can be classified as pulmonary when it only affects the lungs, and extrapulmonary when it involves other parts of the body.
Okay, so all these different TB stages have different clinical manifestations. Generally, clients with primary TB are completely asymptomatic, or may have mild flu-like symptoms like fever, fatigue, malaise, night sweats, anorexia and unintentional weight loss, and a persistent cough. In addition, some clients may experience dyspnea and hemoptysis. Latent TB is always completely asymptomatic, and clients at this stage are not contagious.
Now, clients experiencing secondary or primary progressive TB often have similar but more severe symptoms of primary TB, as well as chest pain, and can sometimes progress to pulmonary complications like pleural effusion or even respiratory failure.
Finally, miliary TB may cause additional symptoms and complications, depending on which organs are affected. Kidneys are commonly affected, resulting in sterile pyuria and hematuria, as well as dysuria and even flank pain. It might also spread to the cervical lymph nodes causing painless lymphadenitis in the neck, also known as scrofula; as well as the meninges of the brain, causing meningitis; and the spinal vertebrae, causing Pott disease, characterized by pain, stiffness and even deformity.
Now, diagnosis of TB begins with the client’s history and physical assessment. Auscultation of the lungs may reveal bronchial breath sounds, crackles, or dullness with percussion over the affected areas. This can be followed with screening tests for TB.
The most common test is the purified protein derivative or PPD skin test, also known as a tuberculin skin test or the Mantoux test; where a mycobacterial protein called tuberculin is injected intradermally on the ventral surface of the forearm and then checked within 48 to 72 hours. If the client has previously been exposed to TB, the immune system reacts to tuberculin and produces a small, localized skin reaction, which is considered a negative result; if the reaction creates induration, so a hardened raised area that is palpable, rather than just redness, the test is positive. The induration should also be measured in millimeters. An induration that’s 15 millimeters or larger is considered positive in all clients; while an induration that’s 10 millimeters or larger is considered positive in clients from endemic countries, as well as those who live or work in high risk settings, those who abuse illicit drugs, or have underlying medical conditions that put them at higher risk, such as diabetes, and children. Lastly, an induration that’s 5 millimeters or larger is considered positive in immunocompromised clients, such as those with HIV, as well as in clients who had recent contact with an infected person.
However, a positive tuberculin test simply means the individual has been exposed to the TB bacteria at some point. It doesn’t differentiate between active, latent or resolved infections, and there’s also the chance of false positive results in vaccinated clients. On the other hand, clients who get a negative test result may get a two-step tuberculin skin test, meaning that a second test is performed after 7 days to rule out a false negative.
An alternative test is the interferon gamma release assay, or IGRA for short, which is a blood test that measures the amount of interferon-gamma released by T-lymphocytes when exposed to mycobacterial antigens, and is less likely to give false positive results.
If any of the two tests is positive and the client presents characteristic TB symptoms, the next step is a chest X-ray to confirm the diagnosis and look for signs of active TB like Ghon lesions. If chest X-rays are positive, it’s important to collect three samples of sputum or bronchoalveolar lavage. These samples are sent to the lab for staining, culture, and nucleic acid amplification tests to look for evidence of acid fast mycobacteria. Finally, a lung biopsy can be performed, which can reveal Ghon lesions.
Key Takeaways
Tuberculosis (TB) is a chronic infectious disease caused by the bacterium Mycobacterium tuberculosis. It primarily affects the lungs but can also spread to other parts of the body. TB is transmitted through the air when an infected person coughs, sneezes, or talks, and another person inhales the bacteria.
People with active tuberculosis infections may experience flu-like symptoms, as well as chest pain, or even respiratory distress. Treatment for TB requires long-term antibiotics, often for 4 months to one year.
The goals of nursing care include improving the client's pulmonary function, providing supportive care during treatment, and preventing the spread of TB to others. Client and family teaching focuses on adherence to their medication regimen, infection control measures, and when to contact their healthcare provider.