Congenital heart defects - Cyanotic: Nursing
Introduction0:00–0:40
Congenital heart defects are cardiac conditions and anomalies that are present at birth. These are usually divided into two categories based on the presence or absence of cyanosis, which means bluish discoloration of the skin.
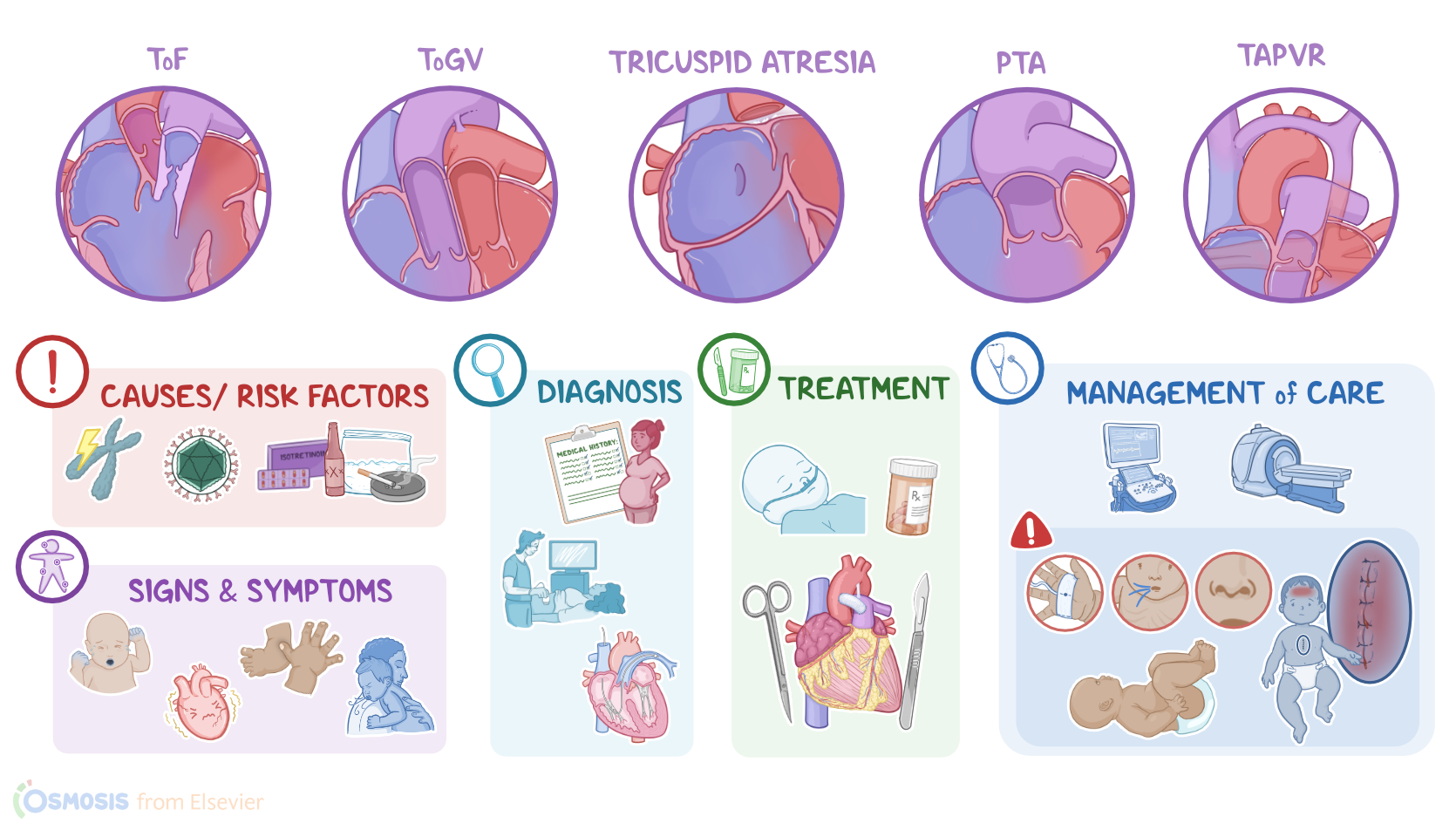
The main types of cyanotic heart defects are tetralogy of Fallot, or ToF for short, which is the most common one; in addition to transposition of great vessels, or ToGV; tricuspid atresia; as well as persistent truncus arteriosus, or PTA; and total anomalous pulmonary venous return, or TAPVR.
Now, let’s quickly recap the anatomy and physiology of fetal circulation. During fetal life, the lungs are filled with fluid and have high vascular resistance, so they don’t participate in gas exchange.
Physiology0:40–3:41
Instead, the placenta serves as the organ of gas exchange, as well as delivering nutrients and removing metabolic wastes from the fetus.
So, oxygenated blood flows from the uterine arteries into the placenta, where oxygen passes through the capillaries and into the umbilical vein.
Then, part of the blood reaches the fetal liver, whereas about half of it bypasses the liver by a shunt called the ductus venosus, which diverts the oxygenated blood into the inferior vena cava, which has deoxygenated blood from the lower body.
Then, this blood flows into the right atrium and further mixes with deoxygenated fetal blood coming from the brain and upper body through the superior vena cava.
Most of this mixed blood then moves through a small flap called the foramen ovale directly into the left atrium, into the left ventricle, and through the ascending aorta into the systemic circulation, supplying oxygen to the brain and upper body, as well as the lower body.
The rest of the blood from the right atrium flows into the right ventricle, and into the pulmonary arteries. A small amount of this blood moves into the pulmonary circulation and perfuses the lung tissue, but most of it is shunted through the ductus arteriosus back into the aorta and systemic circulation.
Ultimately, the blood flows from the systemic circulation into the umbilical arteries, and then back to the placenta. At birth, when the umbilical cord is cut, the baby stops receiving oxygenated blood from the placenta.
As a result, the baby’s blood has a reduction in oxygen levels, and an increase in its carbon dioxide levels. This change stimulates the respiratory center in the baby’s brain, which stimulates the newborn to take their first breath, along with temperature changes and tactile stimulation in the extrauterine environment.This prompts a series of changes, which include lung expansion and decreased pulmonary vascular resistance, allowing increased blood flow to the lungs.
In addition, there’s a functional closure of the foramen ovale and ductus arteriosus. With time, the ductus venosus, ductus arteriosus, the umbilical arteries, and the umbilical vein atrophy and convert into ligaments.
Now, the exact cause of congenital heart defects is unknown, but it's believed to be associated with risk factors that can interfere with the development of the heart.
These risk factors include chromosomal abnormalities of the fetus, in addition to maternal infections, chronic illnesses.
and exposure to teratogens. The list of teratogens is long, and it includes things like medications such as isotretinoin, alcohol, recreational drugs like cocaine, tobacco smoke, and heavy metals like mercury.
Causes & risk factors3:41–4:15
The pathology of cyanotic congenital heart defects starts when a cardiac structure fails to form or close properly. The main types of cyanotic heart defects are tetralogy of fallot, or ToF for short, transposition of great vessels, or ToGV, tricuspid atresia, as well as persistent truncus arteriosus, or PTA, and total anomalous pulmonary venous return, or TAPVR.
Pathology4:15–8:11
So, in tetralogy of Fallot or ToF, there are four heart abnormalities: pulmonary stenosis, which is narrowing of the pulmonary valve; right ventricular hypertrophy, which is enlargement of the right ventricle; ventricular septal defect, which is a gap in the ventricular septum that separates the right and left ventricles; in addition to overriding aorta where the aorta is shifted and sits above the ventricular septal defect.
So the result is oxygen rich blood and oxygen poor blood in the right and left ventricle mix due to the ventricular septal defect, and then it’s pumped out of the overriding aorta.
Next is transposition of the great arteries, or TGA, where the aorta and the pulmonary trunk swap locations. When this occurs, oxygen poor blood returning to the right side of the heart is pumped into the aorta and the rest of the body instead of the pulmonary artery and the lungs.
With tricuspid atresia, the tricuspid valve that normally prevents blood from returning into the right atrium when the right ventricle contracts, is malformed or fails to develop entirely.
Because of this, oxygen poor blood returning to the right atrium can not enter the right ventricle, so an atrial septal defect is needed to mix the blood in the right and left atrium, and a ventricular septal defect is needed for the blood to mix in the right and left ventricle.
Next is persistent truncus arteriosus, where the truncus arteriosus doesn't split properly into the aorta and pulmonary artery during fetal development.
So this extra large vessel sits above both ventricles and allows deoxygenated blood and oxygenated blood to mix before getting pumped to the lungs and the rest of the body.
Finally, there’s total anomalous pulmonary venous return , or TAPVR, in which all four pulmonary veins form abnormal connections.
So instead of returning blood from the lungs to the left atrium, they connect to the right atrium, the superior vena cava or inferior vena cava.
The result is that oxygen rich blood from the lungs returns to the right side of the heart, where it’s pumped back to the lungs.
The condition is only compatible with life if there’s an atrial septal defect that allows some of the blood in the right atrium to flow into the left atrium where it could eventually be pumped into systemic circulation.
Regardless of the type of defect, the blood being pumped out of the heart does not contain enough oxygen to adequately supply the body tissue, leading to cyanosis.
In terms of complications, the persistence of deoxygenated blood in systemic circulation can progress to chronic hypoxia, to which the body responds by producing more red blood cells, called polycythemia.
The heart can also fail to pump enough oxygenated blood to the tissues, resulting in heart failure. At the same time, if the oxygen supply to the brain gets so low, it may result in a cerebrovascular accident, or CVA for short.
Other complications of cyanotic heart defects include arrhythmias, embolism, and infective endocarditis, brain abscess formation, pulmonary vascular disease, and even death.
Clinical manifestations of cyanotic heart defects mainly include cyanosis, which is typically present at birth or within the first few weeks of life.
This is often joined by lethargy, tachycardia, tachypnea, activity intolerance, as well as clubbing of fingers and toes.
Some clients may also experience feeding problems, which may lead to poor weight gain, and failure or difficulty to thrive.
Clinical manifestations8:11–9:49
Clients with Tetralogy of Fallot, can have acute and severe cyanotic episodes, called “Tet spells”. This is where activities like feeding, exercise, or crying, cause spasm of the infundibular septum which worsens the stenosis and increases the obstruction to pulmonary blood flow.
This is called right ventricular outflow tract obstruction and results in increased right to left shunting, eventually decreasing the blood flow through the lungs, causing a fall in arterial oxygen saturation.
The lack of oxygen causes tachypnea or rapid abnormal breathing; and increases the activity of the sympathetic nervous system, eventually increasing heart contractility and even more obstruction of the right ventricular outflow tract.
As a result, cyanosis occurs. Additionally, clients undergoing a tet spell can be seen squatting or assuming a fetal position.
This position increases the peripheral vascular resistance by kinking the femoral artery, which improves the pulmonary blood flow and relieves the client.
During auscultation of the heart, large defects can be heard as murmurs, from blood moving through the defect. The diagnosis of cyanotic heart defects starts with the mother’s history during pregnancy and physical assessment of the client, followed by echocardiography to visualize the defect.
Most defects can also be detected prenatally by standard obstetric ultrasound examination. Other tests include angiography and pulse oximetry.
Imaging tests, such as echocardiograms, chest X-ray and MRI can identify structural abnormalities; in Tetralogy of Fallot a classic sign found on X-ray is an enlarged, boot-shaped heart.
Diagnosis9:49–10:37
ECG should be done to look for arrhythmias. Finally, cardiac catheterization is sometimes performed to assess the extent of the defect.
Now, the treatment of cyanotic heart defects depends on the type of defect, but starts with oxygen supplementation. If heart failure has developed, medications are needed, including digoxin and diuretics.
Prophylactic antibiotics should also be prescribed to prevent infective endocarditis. Some clients will also benefit from prostaglandin E1 infusion, which can keep the ductus arteriosus open, allowing blood from the pulmonary artery and aorta to mix, which increases the oxygen level of the blood going to the rest of the body.
Treatment10:37–11:36
Finally, definitive treatment consists of surgical correction of the defect, particularly in early infancy or during the first year of life.
Alternatively, a palliative shunt might be performed, which is a surgical procedure in which the aorta is connected to the pulmonary trunk, in order to increase the pulmonary blood flow.
In severe cases, heart transplantation might be required. Alright, let’s look at the nursing care you’ll be providing for your infant with the cyanotic congenital heart defect, tetralogy of Fallot.
Your priority nursing goal is to assist in maintaining adequate oxygenation. Begin by assessing the infant’s oxygenation by initiating pulse oximetry, and assessing their vital signs, respiratory effort, and skin color.
Management of care11:36–13:34
Immediately report to the healthcare provider signs of respiratory distress, such as tachypnea, nasal flaring, retractions, grunting, decreased oxygen saturation, and cyanosis.
Then, provide supplemental oxygen, which will help dilate the pulmonary vasculature; establish IV access and infuse the ordered fluids to increase right ventricular filling and pulmonary blood flow; and prostaglandin E1 to maintain ductal patency and promote pulmonary blood flow.
Be sure to take steps to decrease the risk of hypercyanotic episodes, or tet spells, by maintaining a calm, therapeutic environment to prevent agitation.
If a tet spell occurs, place the infant into a knee-chest position, which will increase systemic vascular resistance and promote systemic venous return to the right side of the heart and into the pulmonary circulation.
Continue to monitor them closely, and immediately report if the tet spell persists. Then, administer the prescribed medications, including morphine, which will provide sedation, as well as beta blockers, to and relax the outflow tract of the right ventricle and promote pulmonary blood flow.
If these interventions don’t resolve the cyanosis, administer the prescribed phenylephrine which will improve outflow from the right ventricle to the lungs.
When the infant is stable, assist with preparing them for complete repair of the heart defect. Now, moving on to client and family teaching.
First, teach the infant’s caregivers that Tetralogy of Fallot is a combination of four heart defects, where the heart pumps oxygen-poor blood to the rest of the body.
Explain that this causes cyanosis, where their baby’s skin and lips, and even their fingernails and toenails turn blue because of lack of oxygen.
General client & family teaching13:34–16:12
Then, talk to them about how their baby may sometimes experience a sudden episode of severe cyanosis, called hypercyanotic or “tet” spells, usually when their baby becomes irritable or cries.
Show them how placing their baby in a knee-chest position can help resolve the cyanosis by increasing blood flow to the lungs.
Then, explain the plan of care, reinforce information about the surgical repair of the defect, and leave plenty of time to answer questions.
When their baby is ready to be discharged, teach them how to provide care at home after surgical repair. Talk to them about the importance of keeping the incision clean and dry, and to monitor the incision site for signs of infection.
Tell them to seek medical attention right away if they notice signs of an infection, such as a fever, excessive drainage, redness, increased pain, or swelling at the incision site.
Next, remind them that their baby will need lifelong monitoring and care, stress the importance of keeping all their baby’s regular appointments with their pediatrician and cardiologist.
As their baby grows, they will need routine tests like ECGs to monitor the heart rhythm, echocardiograms to monitor the circulation around the heart, as well as cardiac magnetic resonance imaging to get a close look at the heart chambers, and additional testing to measure right and left ventricular function.
Lastly, let them know that monitoring of their baby’s motor and neurocognitive development is an important part of their baby’s ongoing care.
Be sure to connect the family to community resources and support groups for others who are parenting a child with a congenital heart defect.
Finally, recommend that the caregivers learn how to provide infant CPR in case of emergency. Instruct them to seek emergency medical attention right away if their baby become lethargic, cyanotic, feeds poorly, or has trouble breathing.
Alright, as a quick recap…. Cyanotic congenital heart defects develop secondary to abnormalities present at birth.
The main cyanotic congenital heart defects are tetralogy of fallot, transposition of great vessels, tricuspid atresia, persistent truncus arteriosus, and total anomalous pulmonary venous return.
Genetic chromosomal abnormalities of the fetus, chronic conditions, infection and exposure to teratogens of the pregnant female are attributed to the development of cyanotic congenital heart defects.
Review16:12–17:16
Clinical manifestations of cyanotic congenital heart defects include cyanosis,clubbing of fingers and toes, activity intolerance and lethargy, tachycardia, tachypnea, and feeding difficulty that results in failure or difficulty to thrive.
Diagnosis is established prior to birth and definitive treatment involves corrective surgical repair of the defect. The priority nursing goal is to assist in maintaining adequate oxygenation.
General family teaching involves care of the infant after surgical repair of the defect, learning about ongoing care, and when to seek medical care.
| CONGENITAL HEART DEFECTS - CYANOTIC | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below