Eating disorders: Nursing process (ADPIE)
Notes
| EATING DISORDERS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Lily Truitt is a 22-year-old female client with a history of anorexia nervosa who is admitted to the medical psychiatric unit following signs of malnourishment at an outpatient clinic appointment.
Over the last two weeks, Lily has expressed increasing concern about the way she looks. She feels that she is overweight and has been anxious about being seen in class and at social events.
She discloses that she has been restricting her intake and that she hasn’t eaten anything in 2 days.
Eating disorders are mental health disorders characterized by abnormal eating behaviors that can negatively impact a client’s physical and mental health.
They are quite common, especially among young females, usually between 12-25 years of age. However, they can affect anybody, regardless of their sex, age, and social background.
The most common eating disorders include anorexia nervosa and bulimia nervosa.
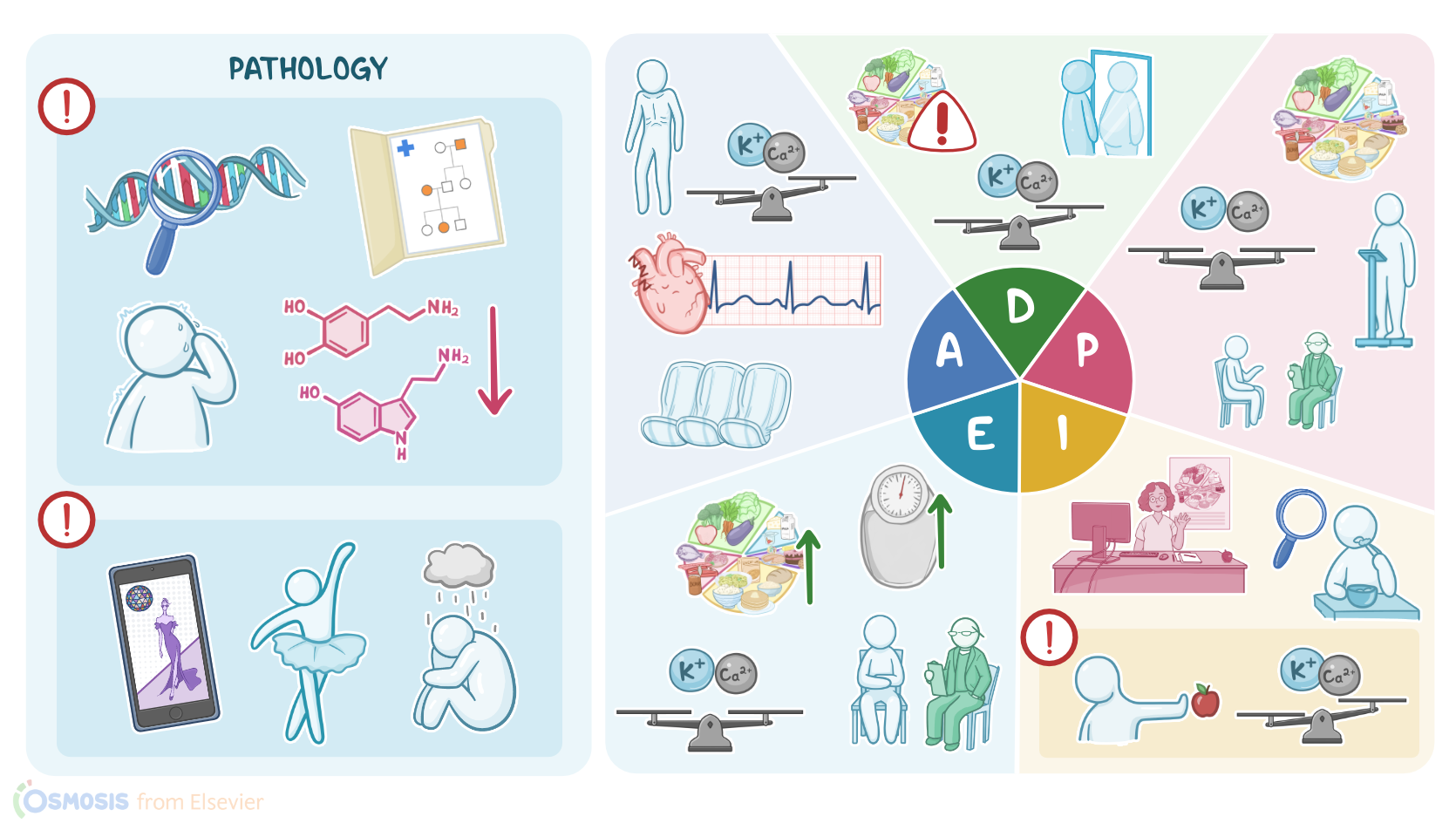
Now, the exact cause of eating disorders is not well known, but they seem to be tied to both biological and environmental risk factors.
Biological risk factors include genetics and family history for an eating disorder, as well as associated mental health disorders like anxiety or obsessive compulsive disorder.
In addition, anorexia nervosa is thought to be associated with dysfunction in neural systems implicated in regulatory self-control and reward, which seems to be caused by a deficiency in neurotransmitters like serotonin and dopamine.
On the other hand, environmental risk factors include the psychosocial pressure to have a socially-defined “ideal body,” and having careers that promote weight loss, like modeling or sports, as well as experiencing childhood trauma, bullying, and loneliness, as well as stress and big life transitions or changes.
Symptoms vary according to the specific eating disorder. Anorexia nervosa is characterized by a constant fear of gaining weight, associated with a distorted body image, with individuals often believing that they are overweight, while actually being underweight, with a Body Mass Index or BMI lower than 18.5.
To avoid gaining weight, clients with anorexia may engage in two main compensatory behaviors. One is the restricting type, where clients reduce the amount of food they eat or over-exercise in order to lose weight without any purging.
The other is the binge-eating and purging type, where clients eat large amounts of food in one sitting and then purge that food through self-induced vomiting or by taking laxatives or diuretics, and this occurs recurrently for at least 3 months.
Now, clients with bulimia nervosa also go through episodes of binge eating followed by compensatory behaviors to prevent weight gain, either by self-induced vomiting, over-exercising, or taking laxatives or diuretics; these episodes repeat consistently at least once a week for a period of 3 months; but still BMI is typically normal or high.
Over time, eating disorders can result in several complications. Clients with anorexia can become severely undernourished, leading to nausea and constipation, as well as amenorrhea and dry skin.
In addition, clients may have bone tissue loss, leading to osteopenia and osteoporosis; and muscle tissue loss throughout the body, which often manifests as fatigue, but can also weaken the diaphragm or the heart, leading to difficulty breathing, bradycardia, and heart or renal failure.
Prolonged food restriction can also lead to dehydration and depletion of electrolytes, which lead to hypotension.
Also, the lack of essential nutrients can lead to iron deficiency anemia, or even pancytopenia. Finally, prolonged anorexia can affect the brain, causing symptoms like confusion, irritability, or restlessness, as well as mental health problems like depression or anxiety.
Ultimately, individuals affected by anorexia nervosa may die from these complications or attempt suicide. With bulimia, repeated vomiting can lead to erosion of the dental enamel, and bilateral sialadenosis, which is the swelling of the salivary glands.
In individuals who use their hand to induce vomiting, the back of the knuckles can get calloused, which is called Russell’s sign.
Forceful vomiting can also lead to Mallory Weiss syndrome, which involves tearing of the distal esophagus and stomach itself, and can cause abdominal pain and hematemesis.
Over time, purging methods can cause dehydration and lead to hypotension, usually combined with tachycardia; as well as depletion of electrolytes, like potassium, or hypokalemia, which is particularly worrisome because it can lead to muscle weakness and even cardiac arrhythmias.
An excessive loss of gastric acid when vomiting might also lead to metabolic alkalosis.
Diagnosis of eating disorders typically involves history and clinical presentation, and is based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, or DSM-5.
However, lab tests can be useful to detect complications, including a complete blood count, coagulation panel, and metabolic profile, as well as electrolyte levels, and liver, kidney, and thyroid function tests.