Gout: Nursing process (ADPIE)
Gout: Nursing process (ADPIE)
Musculoskeletal system
Musculoskeletal system
Notes
| GOUT | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Hubert Symanski is a 49-year-old male client with a history of Type 2 diabetes mellitus who presents to the clinic today with severe pain in the big toe of his right foot.
He explains that when he woke up this morning his toe was red, swollen and felt like it was on fire. He denies any recent injury to his toe or foot.
Walking around the house and putting on shoes is very painful, and the only shoes he can comfortably put on are sandals.
He reports that he had an episode of gout a year ago, confirmed by joint aspiration, and he is concerned that this may be another episode.
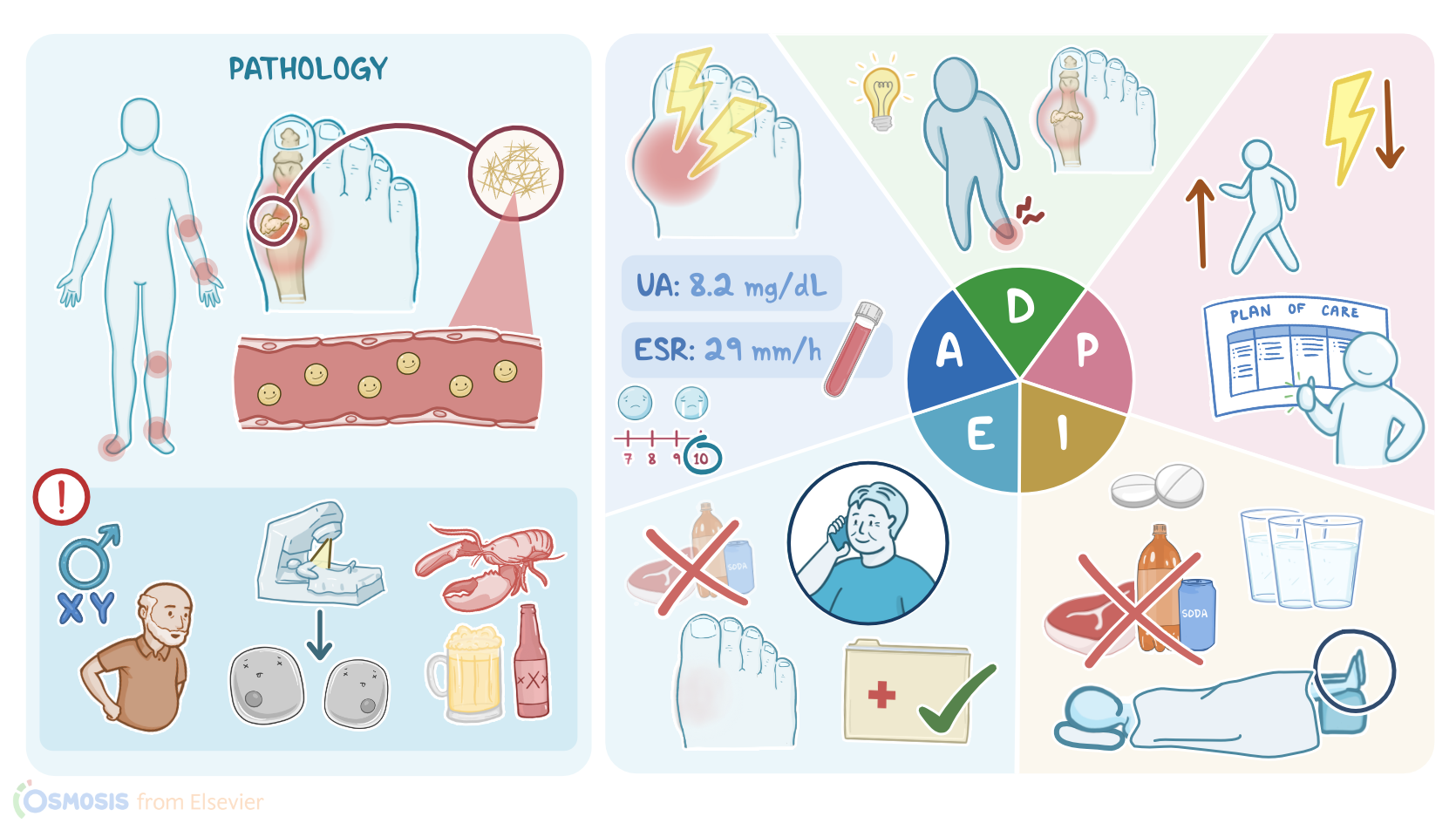
Gout is an inflammatory disease in which urate crystals deposit in a joint and cause damage.
Typically, the underlying cause is hyperuricemia, or too much uric acid, also known as urate, in the blood.
Uric acid is a natural waste product of purines, which are one of the building blocks of DNA and RNA.
Once produced, uric acid circulates in the bloodstream before it is filtered out and excreted by the kidneys to the urine.
Now, hyperuricemia is associated with several risk factors.
An important risk factor is overproduction of purines, which is most common with increasing age, male sex, obesity, and alcohol use.
Overproduction of purines can also occur with increased consumption of purine-rich foods such as shellfish, alcohol, anchovies, and red meat, as well as high-fructose corn syrup containing beverages such as sodas.
Hyperuricemia can also result when cells die at a faster than normal rate, resulting in increased breakdown of purines into uric acid, for instance as a result of chemotherapy, radiation treatment, as well as recent trauma or surgery.
In addition, some individuals have a genetic predisposition to developing hyperuricemia, so an important risk factor is family history.
Finally, hyperuricemia can also occur when there’s reduced excretion of uric acid by the kidney, which can result from dehydration, diabetes, chronic kidney disease, and medications like thiazide diuretics or aspirin.
Now, gout typically presents with acute attacks, in which a joint becomes red, warm, tender and swollen within hours.
Gout can affect many joints, such as those in the ankles, knees, wrists, and elbows, but most often, it affects the first metatarsal joint of the foot, or the base of the big toe, and this is called podagra.
Classically in podagra, the client will wake up from sleep feeling like their big toe is on fire; even the weight of the sheets can be painful!
The pain is most severe in the hours immediately following the gout attack, and then generally lessens over time, but the discomfort and swelling can last for a few days with treatment or weeks without treatment.
Over time, repeated gout attacks can result in chronic gout, which is a type of arthritis with permanent joint destruction and deformity.
Chronic gout can eventually lead to permanent deposits of urate crystals, called tophi, along the bones just beneath the skin.
Individuals with chronic gout are also at an increased risk for developing kidney stones made of uric acid, as well as urate nephropathy, which is when urate crystals deposit in the kidney tubules.
Okay, gout is usually diagnosed based on the client’s history and physical examination.
Laboratory tests may reveal hyperuricemia, or increased blood urate levels, as well as increased C reactive protein or CRP, and erythrocyte sedimentation rate or ESR, which indicate ongoing inflammation.
Diagnosis can be confirmed with a joint aspiration to verify the presence of urate crystals in the synovial fluid.
And in case of chronic gout, imaging techniques like X-rays may detect tophi.
Treatment of a gout attack is focused on decreasing the pain and swelling with NSAIDS, like ibuprofen or naproxen sodium.
Occasionally, corticosteroids like prednisone and antigout agents like colchicine can be used as an alternative to NSAIDs.
After managing the acute attack, clients may also take medications that help decrease uric acid levels, such as xanthine oxidase inhibitors like allopurinol; as well as uricosuric medications, like probenecid, that increase excretion of uric acid by the kidneys.
Finally, it’s important to address the underlying risk factors.
This may include modifying the diet and reducing or eliminating soda, alcohol, red meat, and seafood, as well as staying hydrated, and managing underlying disorders, such as diabetes or chronic kidney disease, and avoiding certain medications like thiazide diuretics.
As you enter the room, you begin your assessment by asking what brings him into the clinic today.
He points to his right toe, which is red and swollen at the first metatarsal joint.
He tells you his toe feels like it is on fire, and that he can hardly walk due to the pain.
You help Mr. Symanski onto the exam table to take a closer look, and observe that he grimaces when bearing weight on his right foot.
Sources
- "Role of diet in hyperuricemia and gout" Best Pract Res Clin Rheumatol (2021)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "The Challenges of Approaching and Managing Gout" Rheum Dis Clin North Am (2019)
- "Gout epidemiology and comorbidities" Semin Arthritis Rheum (2020)
- "The role of diet in hyperuricemia and gout" Curr Opin Rheumatol (2021)
- "Gout and Diet: A Comprehensive Review of Mechanisms and Management" Nutrients (2022)