Hyperemesis gravidarum: Nursing
1,229views
Hyperemesis gravidarum: Nursing
A31- maternal newborn Nursing
A31- maternal newborn Nursing
Notes
| HYPEREMESIS GRAVIDARUM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Nausea and vomiting of pregnancy, or morning sickness, is a common sign of pregnancy. However if there’s more severe and persistent nausea and vomiting it is called hyperemesis gravidarum. This disorder can be dangerous to the mother and fetus if left untreated.
First, let’s quickly review some relevant physiology during pregnancy. There are several hormonal changes, like increased estrogen and progesterone, as well as increased levels of human chorionic gonadotropin, or beta-hCG for short. These changes ensure the normal progression of pregnancy, and also contribute to some maternal physiological changes, such as relaxation of smooth muscles in various parts of the body.
This leads to decreased motility in the gastrointestinal tract so there’s a delay in the movement of food through the stomach and intestines. In addition, relaxation of the lower esophageal sphincter allows stomach acid to reflux up the esophagus. This can cause “heartburn” and sometimes nausea. Due to these changes, many pregnant mothers experience “morning sickness” which is mild and episodic nausea that can appear, despite its name, at any time of the day. It typically starts as early as 5-6 weeks of gestation and ends at 16 to 20 weeks. This is considered a physiological process during pregnancy and is harmless to the mother and fetus.
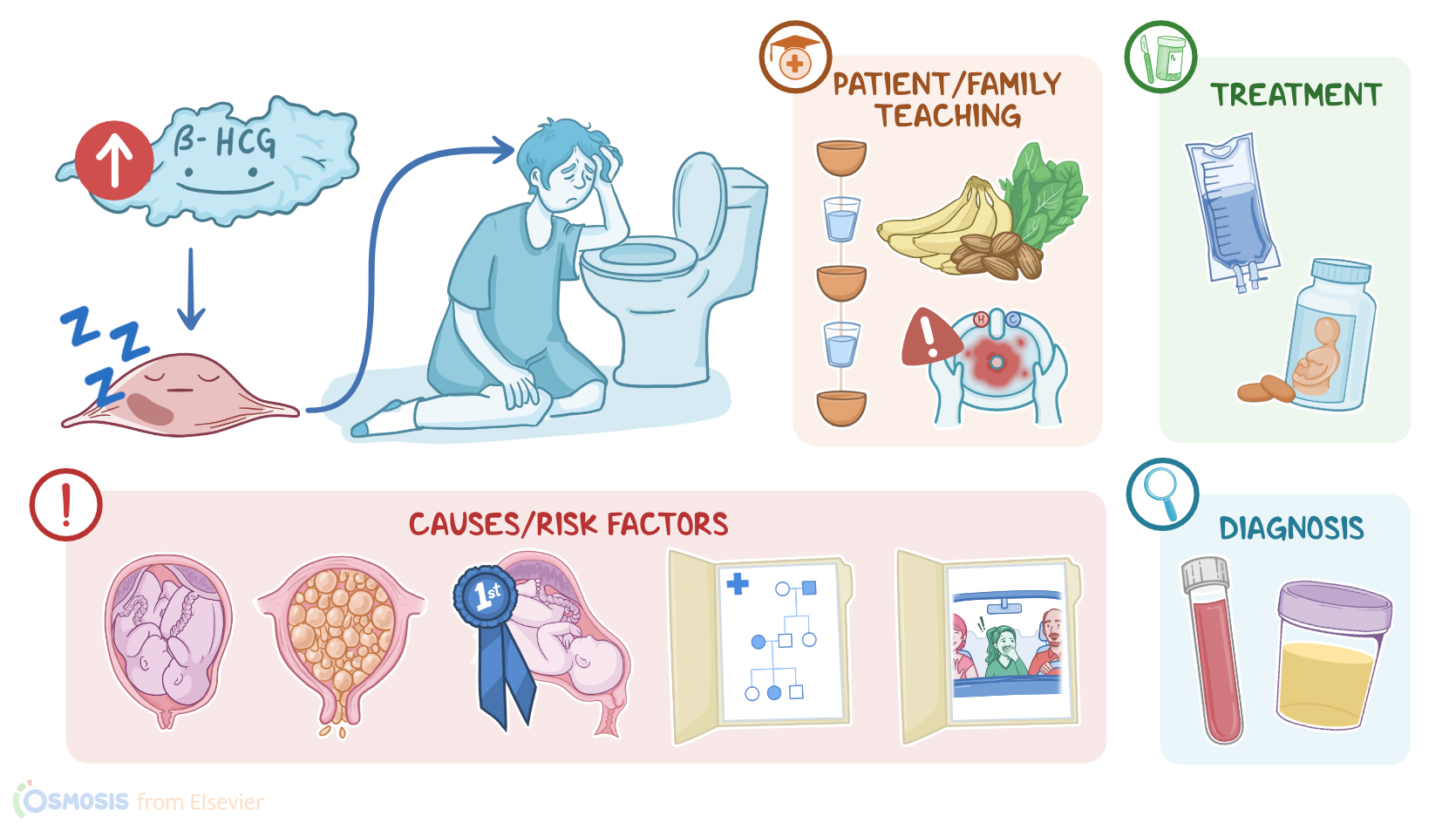
Now, the cause of hyperemesis gravidarum is not fully understood, but it’s thought that some people produce increased levels of estrogen, progesterone and especially beta-hCG or they respond to the increased levels of these hormones more severely.
Some risk factors for hyperemesis gravidarum include conditions that cause an additional increase of beta-hCG levels, like multigestational pregnancy and gestational trophoblastic disease. Other risk factors include being pregnant for the first time, called primigravida, white race, as well as a family history of hyperemesis gravidarum, which suggests a genetic component. Those with a personal history of motion sickness or migraines also seem to be at greater risk of developing hyperemesis gravidarum.
The pathology of hyperemesis gravidarum starts with a genetically susceptible client who is undergoing hormonal changes due to pregnancy. This causes them to experience more severe and persistent nausea and vomiting compared to those experiencing regular morning sickness. Persistent vomiting can impair digestion and lead to malnutrition and weight loss. When the body is energy-starved, it switches to using up all the fat stores for energy; and then moves on to breaking down proteins for fuel. This produces ketones which can be detected in the urine and it’s called ketonuria.
When ketones build up in the blood, it causes acidosis, however the loss of stomach acid with the vomiting could also cause alkalosis. In addition fluid is also lost through the vomit so there’s often dehydration. Other complications include coagulation disorders and hypokalemia. Alternatively, fetal complications include low-birth weight, preterm labor, and intrauterine growth restriction, or IUGR for short.
Clients with hyperemesis gravidarum typically present with nausea and vomiting several times a day, or persist throughout the day. Signs and symptoms of dehydration include weight loss, decreased urinary output, dry skin or mucous membranes, decreased skin turgor, hypotension, tachycardia, and dizziness.
The diagnosis of hyperemesis gravidarum is often based on the client’s history and physical examination only. The diagnosis can be made if pregnancy related nausea and vomiting interferes with their normal daily intake of food or water; interferes with their activity of daily living; or if there’s a weight loss of over 5 percent of prepregnancy body weight.
Laboratory tests can show elevated levels of beta-hCG, and can demonstrate complications like electrolyte and acid-base imbalances, as well as the presence of ketones in the urine.
Treatment of hyperemesis gravidarum starts with dietary changes that decrease the frequency and severity of vomiting, like identifying trigger foods or smells and avoiding those if possible. Additionally, antiemetics, like a combination of doxylamine and pyridoxine, can be given.
Supportive treatment options include intravenous fluid replacement, vitamin and mineral supplementation, or total parenteral nutrition in severe cases. Finally, recent studies have shown that hyperemesis gravidarum can be prevented by preconceptional supplementing with prenatal vitamins for at least one month before conception.
Alright, let’s take a look at the nursing care you’ll be providing for a client with hyperemesis gravidarum. Priority goals of care include initiating measures to reduce vomiting, maintaining fluid and electrolyte balance, and providing emotional support.
First, assess your client’s severity of nausea and vomiting. Ask them about frequency or nausea, how often they vomit, and the color and consistency of emesis. Ask about things that make the vomiting worse or better, and if there are any treatments they have tried.
Then, assess for signs and symptoms of dehydration, including weight loss, decreased urinary output, dry skin or mucous membranes, and decreased skin turgor. Collect laboratory samples, including CBC, CMP, and urinalysis.