Hypothyroidism: Nursing process (ADPIE)
Hypothyroidism: Nursing process (ADPIE)
test 4
test 4
Notes
| HYPOTHYROIDISM | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
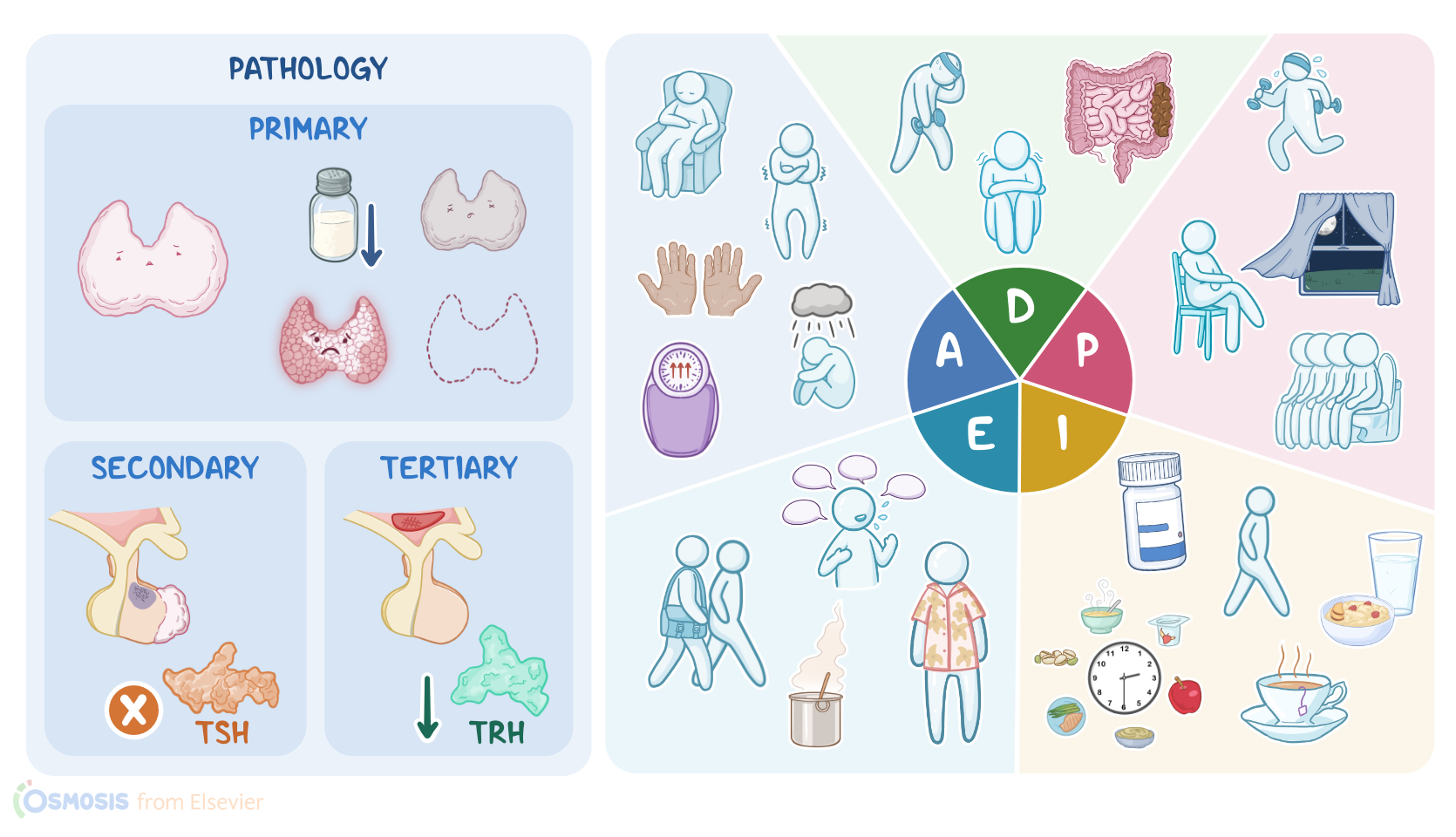
Blythe Callaghan is a 71-year-old female client who presents to the primary care clinic with fatigue, weight gain, and constipation. She also reports feeling cold and depressed and has spent the past few days in bed. After an examination by her physician and a review of laboratory results, Blythe is diagnosed with primary hypothyroidism. Hypothyroidism is a condition in which the thyroid gland produces and releases low amounts of thyroid hormones. Now, hormonal production is normally regulated by the hypothalamus, which is located at the base of the brain. When the hypothalamus detects low blood levels of thyroid hormones, it releases thyrotropin-releasing hormone, or TRH for short. TRH then stimulates the anterior pituitary gland to release thyroid-stimulating hormone, or TSH, which in turn stimulates hormone production by the thyroid gland, a butterfly-shaped gland located in the neck. The thyroid gland is made up of thousands of thyroid follicles, which release two iodine-containing thyroid hormones, triiodothyronine or T3, and thyroxine or T4, into the bloodstream. These hormones then get picked up by nearly every cell in the body. Once inside the cell, T4 is mostly converted into T3, which is the active form. T3 speeds up the cell's basal metabolic rate by stimulating protein synthesis, and burning up more energy in the form of sugars and fats. Other effects of thyroid hormones include increasing the cardiac output, stimulating bone resorption, as well as heat production and activating the sympathetic nervous system, which is responsible for our 'fight-or-flight' response. Now, hypothyroidism occurs when there's low levels of thyroid hormones, which causes a slowing down of metabolic processes. Hypothyroidism is usually either primary, secondary, or tertiary. In primary hypothyroidism, the problem is an underactive thyroid gland. Now, the most common cause of primary hypothyroidism is nutritional iodine deficiency, especially in countries that don't fortify food with iodine. On the other hand, the most common cause of primary hypothyroidism in countries that fortify foods with iodine is Hashimoto thyroiditis, which is an autoimmune disorder against the thyroid gland, ultimately destroying it. Another cause of primary hypothyroidism is thyroiditis, which is an inflammation of the thyroid gland. This may initially cause the release of thyroid hormones resulting in hyperthyroidism. Later on, hormones will be depleted and the gland can no longer keep pace with the damage, which results in hypothyroidism. Finally, primary hypothyroidism can be congenital, also called cretinism, which affects a newborn's central nervous system development. Most of the time it's sporadic, but it can also be caused by an inherited genetic mutation. Ultimately, the newborn's thyroid gland may be absent, underdeveloped, or unable to make enough thyroid hormones. On the other hand, secondary hypothyroidism is usually due to an anterior pituitary gland tumor or infarction, which may prevent TSH production. Finally, tertiary hypothyroidism occurs when there's damage to the hypothalamus due to trauma or compression, leading to decreased TRH production. Now, there are some factors that increase the client's risk of developing hypothyroidism. For Hashimoto thyroiditis, risk factors include female sex, having a family history of Hashimoto thyroiditis, and having personal or family history for another autoimmune disorder like type 1 diabetes mellitus or celiac disease. For thyroiditis, risk factors include viral upper respiratory tract infection, and pregnancy, which may lead to postpartum thyroiditis. Other risk factors for hypothyroidism include certain medications like amiodarone or lithium, as well as radiation therapy for cancers in the neck region. Finally, hypothyroidism can occur following treatment of hyperthyroidism, which may include surgical removal of the thyroid gland, use of radioactive iodine ablation, and the use of antithyroid medications like propylthiouracil and methimazole. Now, symptoms of hypothyroidism include modest weight gain despite a decreased appetite, as well as constipation due to decreased gastrointestinal motility. In addition, clients may experience cold sensitivity because the body is producing less heat. Hypothyroidism also causes bradycardia, fatigue, and shortness of breath. Often, clients may experience forgetfulness and decreased ability to concentrate, as well as paresthesia, or a feeling of 'pins and needles' and numbness involving the limbs. Some clients with hypothyroidism may present with a neck mass due to an enlarged thyroid, known as goiter. In addition, hypothyroidism leads to a build up of glycoaminoglycans in the interstitium of many tissues, resulting in myxedema, or swelling, in the skin and soft tissues like the tongue, as well as the vocal cords, which causes hoarseness. In the skin, the build up of glycosaminoglycans leads to water retention and eventually a non-pitting edema. So, clients may have coarse and doughy skin, resulting in a puffy appearance with periorbital edema and dull facial expressions. In addition, because blood flow to the skin is decreased, the skin becomes cool and dry. Over time, hypothyroidism may result in coarse and brittle hair, which can lead to hair loss. In females, hypothyroidism can cause menstrual cycle irregularities, such as menorrhagia, in which menstrual bleeding is heavy or prolonged; or amenorrhea, where the menstrual cycle is absent. In males, hypothyroidism can cause decreased libido, erectile dysfunction, and delayed ejaculation. If not treated, hypothyroidism can result in complications like anemia, as well as hypercholesterolemia, which can increase the risk of coronary heart disease. Clients may also develop infertility, as well as mental health complications like personality changes and depressed mood. In addition, a significant goiter can compress the trachea, causing difficulty breathing. Finally, one serious complication of inadequately treated hypothyroidism is myxedema coma. This is a medical emergency where the body goes into a state of severe and profound slowing of metabolic processes, leading to cardiovascular collapse. This is usually triggered by acute stress like surgery, infection, and trauma, and presents with hypothermia, hypotension, metabolic abnormalities like hypoglycemia and lactic acidosis, as well as worsening edema, seizures, impaired consciousness, and possibly coma.