Neonatal respiratory distress syndrome (NRDS): Nursing
Neonatal respiratory distress syndrome (NRDS): Nursing
Acute Final
Acute Final
Notes
| NEONATAL RESPIRATORY DISTRESS SYNDROME (NRDS) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
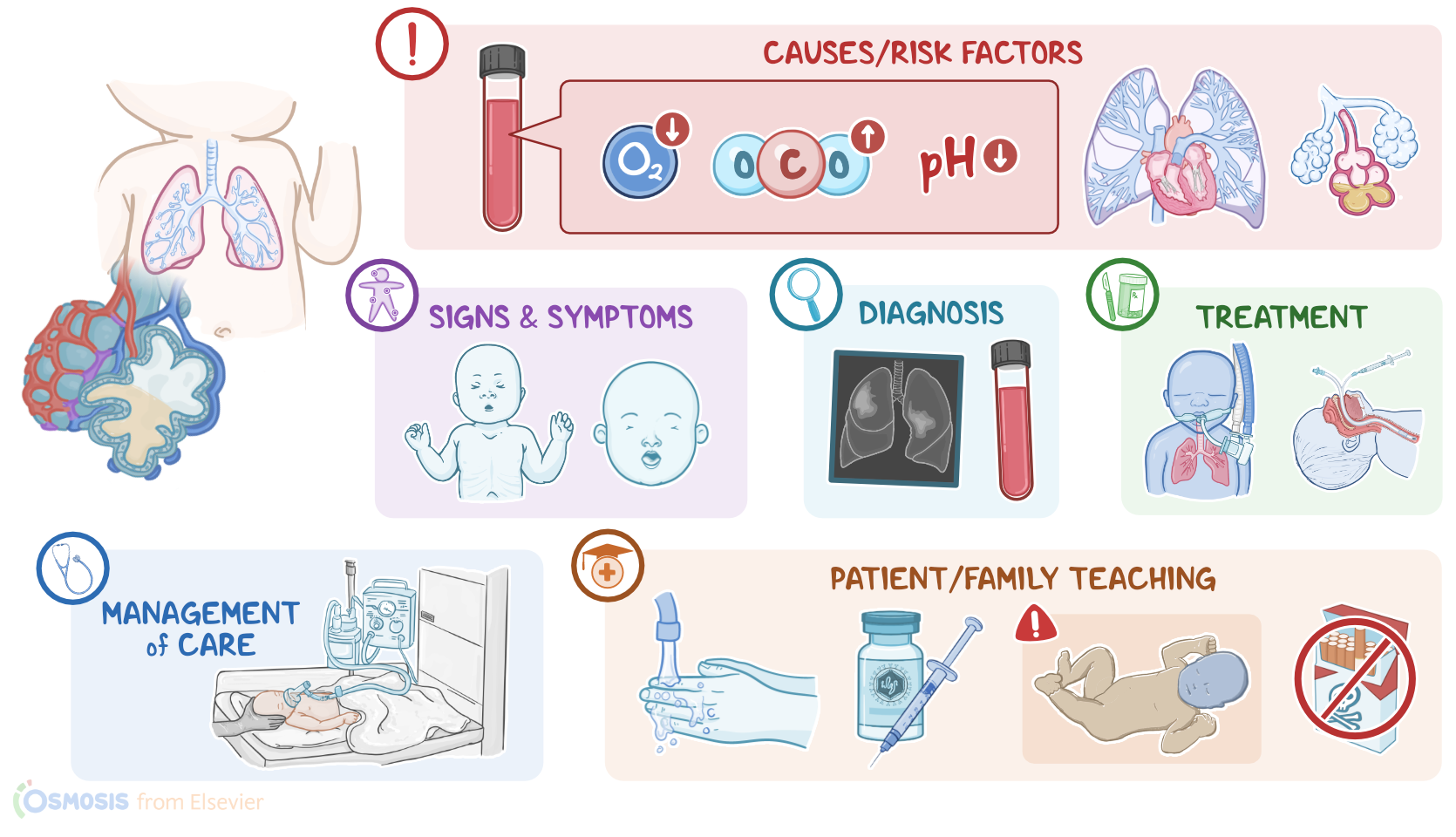
Neonatal respiratory distress syndrome is a respiratory condition caused by deficiency of lung surfactant. It most commonly affects preterm infants, meaning those born before 37 weeks. However, the risk is much higher for those born before the 28th week. The disorder is characterized by alveolar collapse, and noncardiogenic pulmonary edema, which can lead to hypoxemia and respiratory failure.
Alright, now let’s quickly review the physiology of the respiratory system. Alveoli are tiny air-filled sacs where most gas exchange occurs, so as a person breathes, the inhaled oxygen moves from the alveolar sacs into the blood, while the carbon dioxide moves from the blood into the alveolar sacs to be exhaled. During intrauterine life, the alveoli are filled with fetal lung fluid, which expands the lungs and allows them to develop properly. By 24 to 25 weeks of gestation, surfactant production starts.
This is an oily secretion that coats the interior of the alveoli and reduces surface tension to prevent their collapse. Surfactant typically builded up to an adequate level by 34 to 36 weeks of gestation, but more surfactant can also be released during labor and immediately after birth to enhance the transition from fetal to neonatal life. Additionally, with labor approaching, the amount of fetal lung fluid starts decreasing as it gets absorbed from the alveoli into the interstitial space.
Now, at birth, several, mechanical, thermal, and sensory factors stimulate newborns to take the first breath. This allows them to force out the remaining fetal lung fluid and get air to enter the lungs. Infants crying also helps raise the pressure inside the chest, allowing more fluid to exit the lungs. Complete absorption of fetal lung fluid may take several hours after birth.
Okay, now the main cause of neonatal respiratory distress syndrome is insufficient production of lung surfactant, which can be due to premature birth or an abnormal pulmonary surfactant B gene, which is inherited in an autosomal recessive pattern.
Risk factors for the development of neonatal respiratory distress syndrome include prematurity especially in infants born before the 28th week of gestation, and cesarean delivery without labor. Other risk factors include birth asphyxia, where the infant’s oxygen supply is cut off right before, during, or after birth; cold stress; multiple gestation; as well as maternal diabetes. Finally, respiratory distress syndrome is more common among infants assigned male at birth.
Okay, now the pathology of neonatal respiratory distress syndrome starts with insufficient production of surfactant, which causes the alveoli to collapse. At the same time, widespread alveolar collapse leads to damage of the respiratory epithelium, which triggers an inflammatory response in the lungs. This causes capillaries to become permeable to larger molecules like proteins, which leak into the alveoli, pulling water with them, and further inactivating surfactant. The end result is noncardiogenic pulmonary edema.
Now, these collapsed, fluid-filled alveoli cannot participate in gas exchange. This results in acute hypoxemia, or low oxygen level in the blood, and hypercapnia or high carbon dioxide level in the blood. With hypoxemia, tissues in the body do not get enough oxygen so they have to rely on anaerobic metabolism which produces lactic acid, resulting in metabolic acidosis. The inability to get rid of carbon dioxide results in respiratory acidosis. Now, hypoxemia, hypercapnia, and acidosis will cause pulmonary vasoconstriction, which may eventually progress to pulmonary hypertension. With persistent pulmonary hypertension, the ductus arteriosus remains open, resulting in intrapulmonary shunting and decreased oxygenation. Ultimately, the infant may develop complications like respiratory failure and even death.
Clinical manifestations of neonatal respiratory distress start within the first hours after birth, and include nasal flaring, tachypnea, and intercostal or substernal retraction during inspiration, along with grunting during expiration. An asynchronous breathing pattern that creates a paradoxical seesaw respiration pattern between the chest and abdomen may also be seen. During auscultation of the chest, there are typically decreased breath sounds, as well as diffuse crackles which is the sound of collapsed alveoli popping open with inspiration. Signs of impending respiratory failure include gasping and a decreasing respiratory rate.
The diagnosis of neonatal respiratory distress syndrome starts with the client’s history and physical assessment, followed by a chest x-ray or CT scan, which show signs of hypoventilation, such as reduced lung volume, as well as diffuse, reticulogranular ground glass opacities on both lungs. Another feature is air bronchogram where the air-filled bronchi appear dark in contrast to the surrounding white or gray atelectatic tissue.
Arterial blood gas, or ABG analysis may show hypoxemia, hypercapnia and respiratory acidosis. Hypoglycemia will be present due to increased glucose consumption related to prematurity and increased work of breathing.
Treatment of neonatal respiratory distress syndrome starts with administration of warm, humidified oxygen by continuous positive airway pressure or CPAP, using face mask or nasal prongs, along with supportive measures, including stabilization of body temperature, administration of IV fluids, blood glucose stabilization, and nutritional support. Surfactant administration can be given in the delivery room or within the first few hours of life to avoid progressive alveolar atelectasis. In severe cases, intubation and mechanical ventilation might be necessary.
It's important to keep in mind that some of these interventions can cause additional complications. Long-term supplemental oxygen, especially at high concentrations can cause retinopathy of prematurity, pneumothorax, and bronchopulmonary dysplasia, which is a chronic lung disease in which bronchi are damaged and alveolar tissue is destroyed.
Okay, now let’s talk about the care you’ll be giving to a client with neonatal respiratory distress syndrome. Your priority nursing goals are to support respiratory function, provide supportive therapies, and monitor for complications.