Physiologic changes - Pregnancy: Nursing
2,398views
Notes
| PHYSIOLOGIC CHANGES - PREGNANCY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| SIGNS AND SYMPTOMS |
| |
| CARDIOVASCULAR CHANGES |
| |
| RESPIRATORY CHANGES |
| |
| GI AND NUTRITION CHANGES |
| |
| RENAL CHANGES |
| |
| MUSCULOSKELETAL CHANGES |
| |
| REPRODUCTIVE CHANGES |
| |
| ENDOCRINE CHANGES |
| |
| SKIN CHANGES |
| |
Transcript
Physiological changes in pregnancy include all adaptations of the human body that occur in response to a developing fetus. These changes are essential for fetal survival and are primarily caused by high levels of estrogen and progesterone in the body.
First, let’s cover the most important signs and symptoms of pregnancy, which can be subdivided into three main groups: presumptive, probable, and positive. Presumptive signs and symptoms include amenorrhea, or the absence of menstruation; increased breast size and breast tenderness; nausea and vomiting; as well as increased urinary frequency; and quickening, meaning the fluttering sensation caused by fetal first movements.
Probable signs of pregnancy include a positive pregnancy test, uterine enlargement, and irregular uterine contractions, which are often referred to as Braxton Hicks contractions. Other important probable signs include the Goodell’s sign, or the softening of the cervix that occurs after 4 gestational weeks; the Hegar’s sign, which indicates the softening of the lower uterine segment that occurs after 6 gestational weeks; and finally, the Chadwick’s sign, which describes the blue to purple discoloration of vulvar, vaginal, and cervical mucous membranes. Just like Hegar's sign, Chadwick's sign also appears after 6 weeks of gestation.
Another important probable sign is ballottement. Here, an examiner places a finger inside the vagina and pushes the lower segment of the uterus, indirectly pushing the fetus to go upwards. Once displaced, the fetus returns to its previous position causing an impact on the uterine wall. This impact can be felt on the examiner’s finger.
Finally, we have positive signs of pregnancy, which include active fetal movements, detection of fetal heart rate, and ultrasound detection of the fetus.
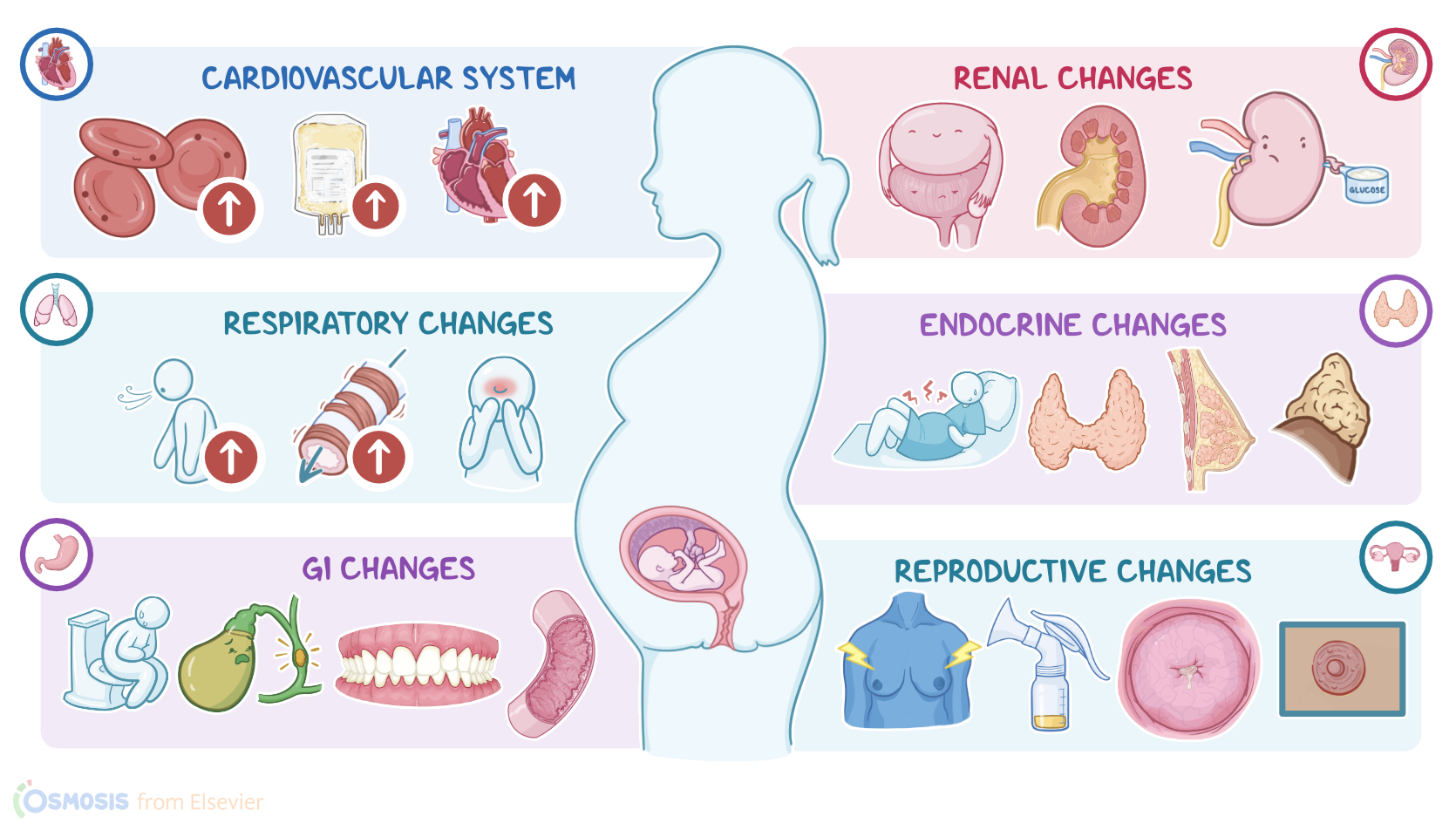
Now, let’s look at the physiological changes that impact the cardiovascular system, which must adapt in order to accommodate the needs of an enlarging uterus and a growing fetus. Pregnancy is called a high volume state because the maternal circulating blood volume increases by 30–50%, which means that blood volume increases from about five liters, in the average individual, to about seven and a half liters by the third trimester. The number of red blood cells increases a bit, but there’s a much larger increase in the plasma volume, which is the portion of blood that doesn’t have red blood cells, which eventually dilutes the blood. As a result, hemoglobin and hematocrit actually go down. This apparent decline in red blood cell levels is called physiological anemia, or pseudoanemia of pregnancy. Similarly, the number of leukocytes increases, but platelets stay within the normal range. However, there’s an increased synthesis of factors that favor blood clotting.
Now, in order to pump all this extra blood to the systemic circulation, cardiac output increases as well, by increasing the number of beats per minute by 10 to 15 bpm, and stroke volume, which refers to the amount of blood pumped with each contraction. In response to the increased workload, the heart size increases. The high volume state can also alter the client’s heart sounds. Finally, as the uterus enlarges, it pushes up on the diaphragm, nudging the heart slightly upward and to the left.
Now, even though there’s an increased circulating blood volume, blood pressure actually falls because increased progesterone and estrogen levels cause vasodilation of peripheral blood vessels and decreased vascular resistance. Now, blood pressure changes are actually minimal when a client is standing or sitting. But, if the client is in the supine position, the weight of the uterus and fetus can compress the large blood vessels, such as the inferior vena cava, decreasing venous return to the heart and cardiac output, causing supine hypotension. More importantly, decreased cardiac output means that the heart pumps less blood into the systemic circulation and the placenta, subsequently causing a deficiency of the uterine circulation that might result in fetal distress. Clients with supine hypotension usually complain of symptoms such as lightheadedness, dizziness, and nausea when lying on their back. To correct this, the client should be turned to a lateral recumbent position, or have a pillow or foam wedge placed under their right lower back. This alleviates the pressure on the vena cava inferior and reestablishes the venous return to the heart.
Now, let’s switch gears and move on to respiratory changes. During pregnancy, oxygen consumption increases by about 15 to 20 percent. The human body adapts to accommodate this by increasing the tidal volume, which is the amount of air inhaled and exhaled per breath, and the respiratory minute volume, which refers to the amount of air inhaled or exhaled per minute. Additionally, high progesterone levels increase the sensitivity of the respiratory center in the medulla oblongata and at the same time, decrease airway resistance.
On the other hand, estrogen does not increase respiratory function, instead, it increases the blood flow through the mucous membranes of the upper respiratory tract. This can result in nasal and sinus stiffness, nosebleeds, and deepening of the voice. Increased blood flow can result in edema of the eustachian tubes and eardrums and cause a sense of fullness in the ears. Finally, as the uterus enlarges, it pushes the diaphragm up around 4 centimeters, which can make it more difficult for the lungs to expand, causing shortness of breath. This can cause the client to compensate by hyperventilation.
Next up are the gastrointestinal changes. Let’s start with the mouth, where estrogen increases the blood flow and causes mucosal hyperemia. Hormonal changes also increase the inflammatory response to dental plaques, which can result in severe gingivitis and gingival bleeding. In the esophagus, progesterone decreases the tone of the lower esophageal sphincter, thereby increasing the risk of gastric reflux and heartburn. Hormonal changes during pregnancy also decrease the tone and motility of the gastrointestinal tract, thereby delaying the emptying of the gastrointestinal content. Furthermore, a decrease in motility gives the intestines enough time to absorb necessary nutrients from the gastrointestinal lumen. On the other hand, decreased motility can also cause bloating, abdominal distension, and constipation. Finally, just like the rest of the gastrointestinal tract, the gallbladder is hypotonic, therefore it requires more time to empty. As a result, the bile becomes thicker, which increases the risk of gallstones.
As far as the nutritional needs go, during pregnancy, clients need to increase their caloric intake by around 300 calories per day. In addition, more protein, calcium, vitamins like folate, and minerals like iron are needed to meet the needs of the growing fetus. Of note, folate supplementation is especially important for the prevention of neural tube defects in the fetus. Luckily, an extra 400 micrograms of folate per day can be found in various prenatal vitamins, and this is just about enough!
Ok, now, let’s look at the renal system changes. Increased cardiac output means that there is more blood going through the kidneys, so they work harder to remove both maternal and fetal waste products. At the same time, the renal threshold for glucose, meaning the blood glucose levels above which glucose is excreted into urine, is lowered, which can sometimes cause glycosuria. Overall, these adaptations make the renal pelvises, calyces, and ureters dilate, resulting in physiologic hydronephrosis and hydroureter.