Preterm labor: Nursing
Preterm labor: Nursing
Maternal/Fetal
Maternal/Fetal
Notes
| PRETERM LABOR | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
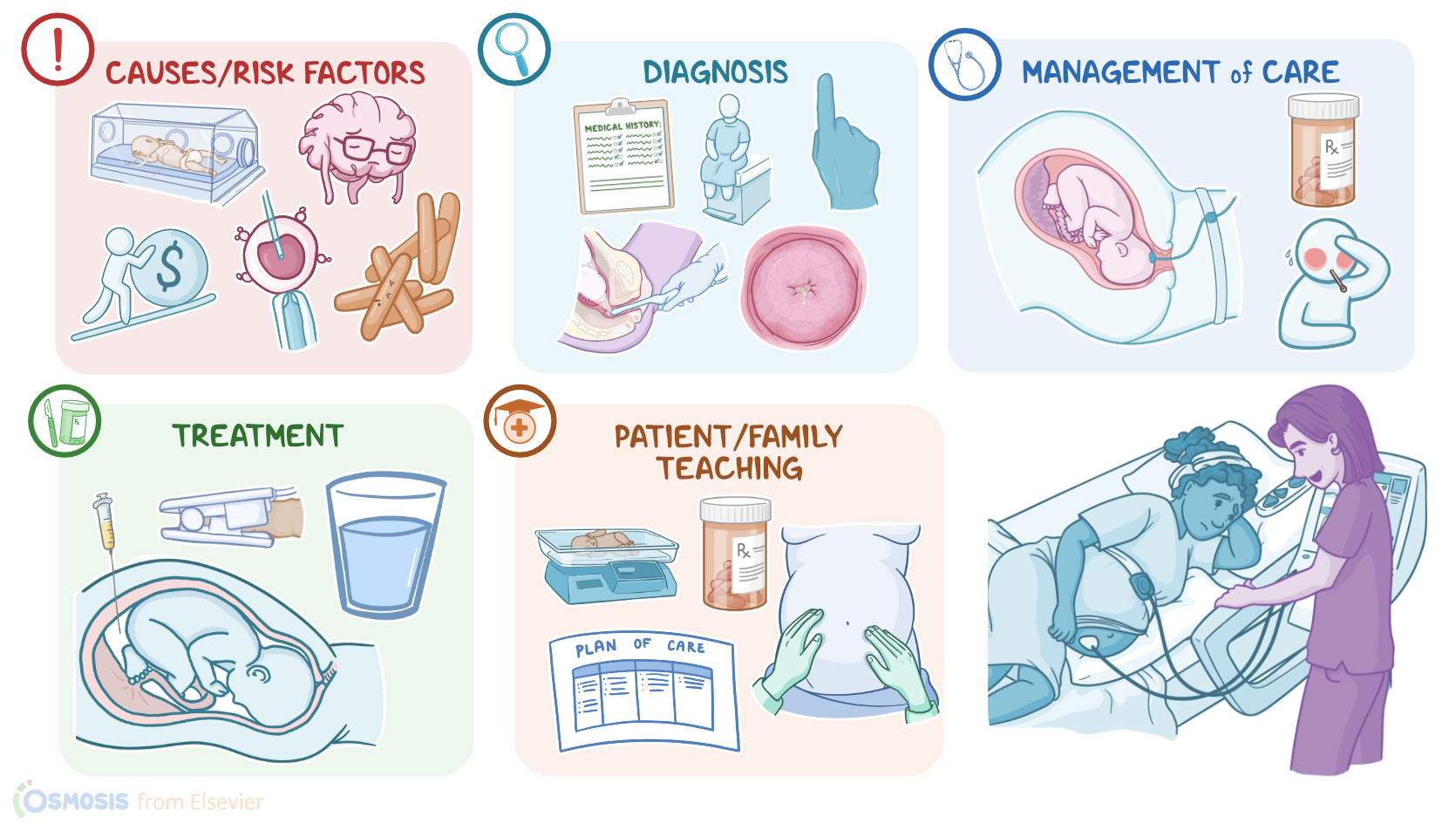
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Labor refers to uterine contractions and cervical changes that lead to childbirth, and this usually occurs between 37 and 42 weeks of gestation. So preterm labor is when labor occurs before 37 weeks gestation.
Okay, now, let’s start by looking at the physiology of labor, also called parturition. This process starts with the release of uterotropins like estrogen which makes the uterine smooth muscles more responsive to stimulation. The stimulation comes from uterotonic compounds like oxytocin and prostaglandin which can induce labor by causing uterine smooth muscle contraction. These contractions are initially mild, short, and far apart, and progress to stronger, longer lasting contractions that are about 3 to 5 minutes apart. The contractions pull back on the tissue of the cervix, causing the membrane to efface and the cervix to dilate.
Now, even though there are several conditions associated with preterm labor, the exact cause isn’t always clear. Stress is one common cause as it can lead to increased prostaglandin production and induce labor early on. This stress can be psychosocial, as well as biological, like when there’s an infection. Certain bacteria can also release toxins that either stimulate uterine contraction or erode the fetal membranes, causing premature rupture of the membranes.
The strongest risk factor for preterm labor is previous preterm labor and birth. Other risk factors include polyhydramnios, meaning excessive amniotic fluid, or oligohydramnios, which is too little amniotic fluid; any structural abnormality of the uterus; in vitro fertilization; multiple gestation; and a history of elective pregnancy termination. Preterm labor is more common in clients with a low socioeconomic status, lack of prenatal care, or if there is heavy alcohol consumption, cocaine use or heroin use, during pregnancy.
Now, whatever the cause, preterm labor before the 34th week of gestation is associated with significantly increased morbidity and mortality. One of the most important causes of morbidity in the fetus is insufficient surfactant production in the lungs, especially before the 28th week. Surfactant is needed to decrease surface tension inside the alveoli and keep them open once the infant is born. If there’s not enough, the infant will develop neonatal respiratory distress syndrome where large numbers of the alveoli collapse after birth leading to impaired gas exchange and respiratory failure.
Another complication is patent ductus arteriosus which is an opening between the pulmonary artery and aorta that would normally close after birth. If the opening persists, blood will move from the aorta into the pulmonary artery, causing systemic hypotension and pulmonary hypertension.
Other complications include hypothermia due to the infant’s inability to produce enough heat, glucose abnormalities, increased risk for infections, hypoxic-ischemic encephalopathy, cerebral palsy, retinopathy of immaturity, and necrotizing enterocolitis. The mother is also at risk for complications. Maternal complications include increased risk of hemorrhage; infection; and complications related to cesarean delivery.
Okay, now, clinically, clients with preterm labor might have light bleeding or vaginal discharge of mucus, which may be clear or slightly bloody. Other times the amniotic membranes might rupture. This is typically followed by the onset of uterine contractions. Other clinical manifestations include a sensation of pressure in the vagina or pelvis, abdominal cramping, and a dull, lower back pain.
The diagnosis of preterm labor starts with the client's history and physical examination. A transvaginal ultrasound can be done to measure the cervical length, amniotic fluid volume, and placental location, as well as fetal presentation and estimated fetal weight. A cervicovaginal discharge sample can be tested for fetal fibronectin, which is a protein that acts like a “glue” between the maternal decidua and fetal membranes. So its presence in cervicovaginal secretions indicates a disruption of these membranes and can be used to predict a higher risk of preterm labor. Preterm labor is confirmed by the presence of regular contractions that result in cervical changes, like dilation, meaning the cervical canal gets wider; and effacing, meaning the cervix gets thinner.
Now, the treatment of preterm labor is determined by gestational age. In pregnancies more than 34 weeks along, delivery is indicated if there are cervical changes, obstetrical complications, or evidence of fetal distress. In pregnancies less than 34 weeks and a high risk of preterm birth, a couple of measures are taken to decrease the risk of neonatal complications. First, since the fetal lungs are not mature, a course of antenatal corticosteroids is given to encourage maturation. In addition, tocolytic or labor suppressive medications, like nifedipine, indomethacin, or terbutaline, are also given to slow uterine contractions and provide the corticosteroids enough time to work; and magnesium sulfate is also given to protect the fetal nervous system, and reduce the risk of cerebral palsy. If bacterial infections are present or suspected, antibiotics are administered.