Renal and urinary calculi: Nursing
1,474views
Renal and urinary calculi: Nursing
N171
N171
Notes
| RENAL AND URINARY CALCULI | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Nephrolithiasis and urolithiasis refer to the presence of stones, also known as calculi, in the kidney and the urinary tract, respectively. Stones form when solutes in the urine precipitate out and crystallize. Depending on which solute precipitates to form the stone, there are five main types of stones: calcium oxalate, calcium phosphate, struvite, uric acid, and cystine stones.
Now, let’s quickly review some anatomy and physiology of the urinary tract, which is made of the kidneys, ureter, bladder, and urethra. The kidneys are in charge of producing urine, which is made up of water and solutes.
The process starts with glomerular filtration in the renal corpuscle, which is made up of the glomerulus and the Bowman’s capsule. As blood flows into the glomerulus, water, electrolytes like sodium, and other small particles in the blood like creatinine, urea nitrogen, and glucose, pass through the endothelial lining of the capillaries and into Bowman's space. Large proteins and red blood cells however, aren’t filtered. Now, the next steps, which include tubular reabsorption and secretion, take place in the renal tubules, which are surrounded by the peritubular capillaries. Here, water and solutes get passed back and forth between the filtrate in the lumen of the renal tubule and the blood in the peritubular capillaries.
Finally, urine is drained into the renal pelvis, which then narrows to form the ureter, and transports urine to the bladder. Ultimately, urine exits the bladder through the urethra.
Now, nephrolithiasis and urolithiasis are caused by the increased concentration of certain solutes in the urine. This can happen if there’s an increase in the solute, which could be calcium with oxalate or phosphate, leading to the formation of calcium stones; magnesium, ammonia, and phosphate, leading to struvite stones, as well as uric acid forming uric acid stones and cystine, forming cystine stones. Alternatively, there could be a decrease in the solvent, or water in the urine.
That being said, the exact cause why these stones form is usually unknown, but they have been associated with several risk factors. Common risk factors for all types of kidney stones include a family history of nephrolithiasis, prolonged immobility, obesity, and dehydration, which is more likely to occur in warm climates or due to low fluid intake.
Now, for calcium stones, risk factors mainly include hypercalcemia and hypercalciuria. This can be a complication of hyperparathyroidism, because parathyroid hormone increases calcium release from the bones and calcium reabsorption from the intestines, while decreasing calcium excretion from the kidneys. Hypocitraturia is another cause, where less citrate is eliminated in the urine. This is because normally, citrate prevents kidney stone formation by inhibiting crystal growth and aggregation.
Additionally, there are medications that can increase the risk of developing calcium stones, like loop diuretics, acetazolamide, theophylline and glucocorticoids. Other risk factors include fat malabsorption, ingestion of ethylene glycol or antifreeze, and high levels of vitamin C, all of which raise oxalate levels in the blood. Finally, a diet heavy in oxalate-rich foods like rhubarb, spinach, chocolate, nuts, and beer increases the risk of calcium stones.
For uric acid stones, risk factors include acidic urine, which can be caused by acidosis, meaning a low blood pH. This can happen with chronic diarrhea, where large amounts of bicarbonate are lost in the stool; or with poorly controlled diabetes, where the body can’t use glucose and instead breaks down fat for fuel, creating acidic ketones as a by-product. Another important risk factor is hyperuricemia, or high levels of uric acid in the blood, which might be due to conditions like gout.
There are also medications that promote the development of uric acid stones, like thiazide diuretics, salicylates, probenecid and allopurinol. Lastly, since uric acid is a breakdown product of purine, consuming lots of purines, which can be found in shellfish, anchovies, red meat or organ meat, increases the risk of uric acid stones.
Next are cystine stones, which occur in the setting of cystinuria, a genetic condition where cystine cannot get reabsorbed from the renal tubules, so instead gets excreted in the urine.
Finally, for struvite stones, the main risk factor is a urinary tract infection with bacteria that produce urease, like Proteus and Klebsiella. These bacteria increase urine pH, making it a favorable environment for magnesium ammonium phosphate to precipitate.
Alright so, pathology of kidney stones begins with urinary supersaturation of certain solutes, which results in precipitation and formation of crystals. Those crystals then act as a nidus, or place where more solutes can deposit, and, over time, this forms a kidney stone. Now, the stone can become stuck and obstruct the urinary tract, which happens most commonly in ureteropelvic junction or in the ureter. When this happens, the ureter becomes dilated and stretched. At the same time, the urothelial lining is damaged, which causes bleeding and consequent hematuria. Also, if the obstruction persists, urine won’t flow, which is called urinary stasis, making the urinary tract prone to infection. Sometimes, kidney stones can completely obstruct the ureter and this way the urine builds up behind the obstruction, causing hydronephrosis, or dilation of the renal pelvis and calyces, which can cause permanent kidney damage.
Key Takeaways
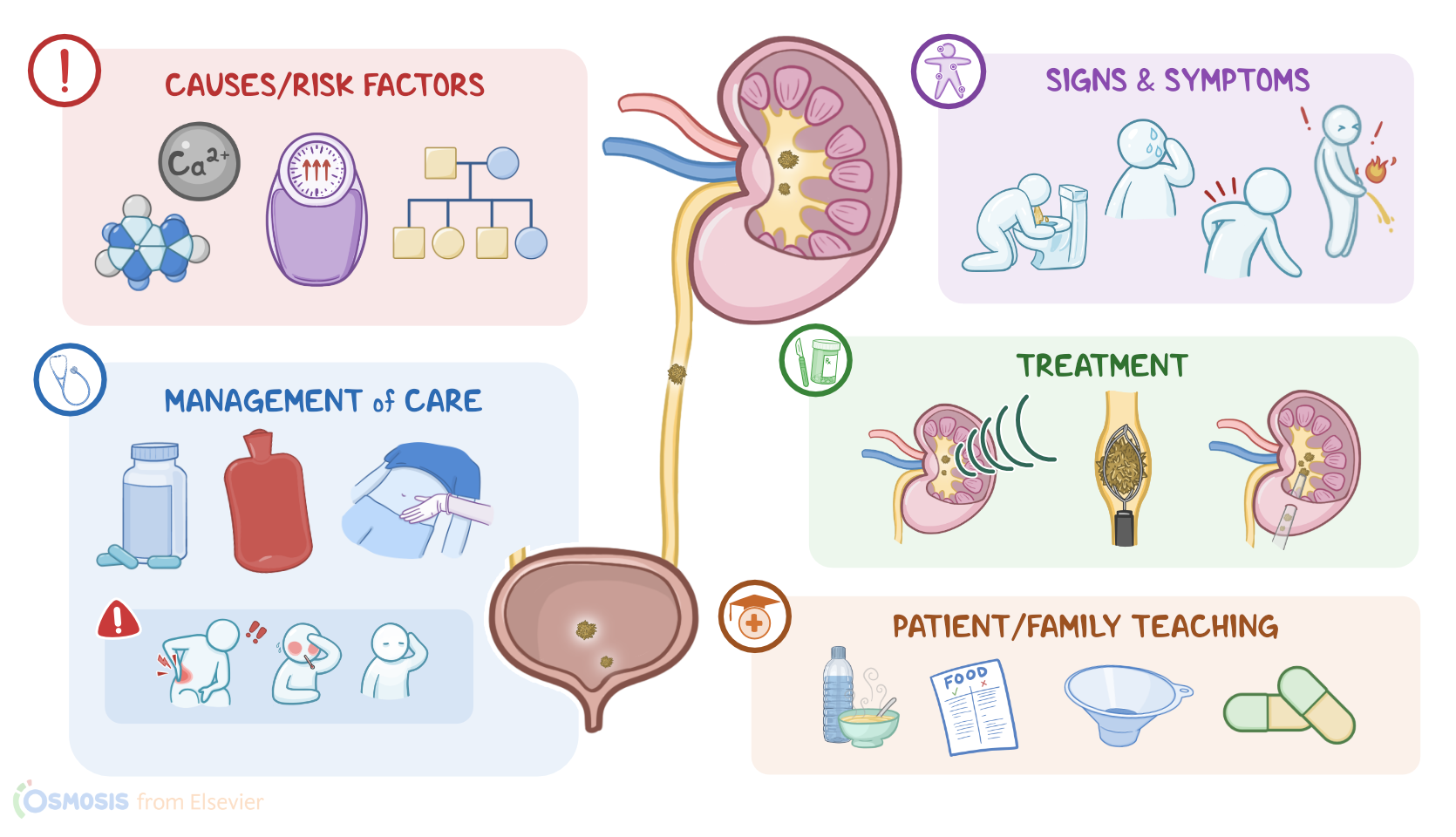
Nephrolithiasis and urolithiasis refer to stones, also called calculi, in the kidney and urinary tract, respectively. They form when solutes in the urine precipitate out and crystallize. Depending on the type of precipitated solute forming the stone, there are five main types of stones: calcium oxalate, calcium phosphate, struvite, uric acid, and cystine stones. Renal and urinary stones can cause urinary tract obstruction, infection, and even hydronephrosis, which can lead to permanent kidney damage.
Even though people with renal and urinary stones may be asymptomatic, common symptoms include renal colic and flank pain. The pain is often sharp, sudden, and severe enough that it may trigger nausea, vomiting, pallor, and sweating. There may also be hematuria, dysuria, urinary urgency and frequency, and signs of infection.
The diagnosis involves a history and physical assessment, followed by lab exams such as urinalysis and blood studies, as well as imaging like CT and ultrasound. Treatment includes medications to treat pain and surgery in some severe cases. There are also other procedures like extracorporeal shock wave lithotripsy (ESWL), which uses high-energy sound waves to break these stones into smaller fragments able to be passed in the urine. Increased fluid intake and dietary changes may be recommended to prevent stone formation in the future.