Reye syndrome: Nursing process (ADPIE)
Notes
| REYE SYNDROME | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Gabriella Jones is a six-year-old girl who was brought to the emergency department by her mother. Mrs. Jones states that for the past 24 hours Gabriella has become increasingly lethargic with rapid breathing and has been vomiting for the past two days.
Mrs. Jones adds that about one week ago, Gabriella had influenza and her pediatrician recommended acetaminophen if Gabriella developed a fever.
Mrs. Jones didn’t have any acetaminophen on hand, so she gave Gabriella two doses of aspirin instead after Gabriella developed a fever. Gabriella is admitted to the pediatric intensive care unit, or PICU, with a probable diagnosis of Reye syndrome.
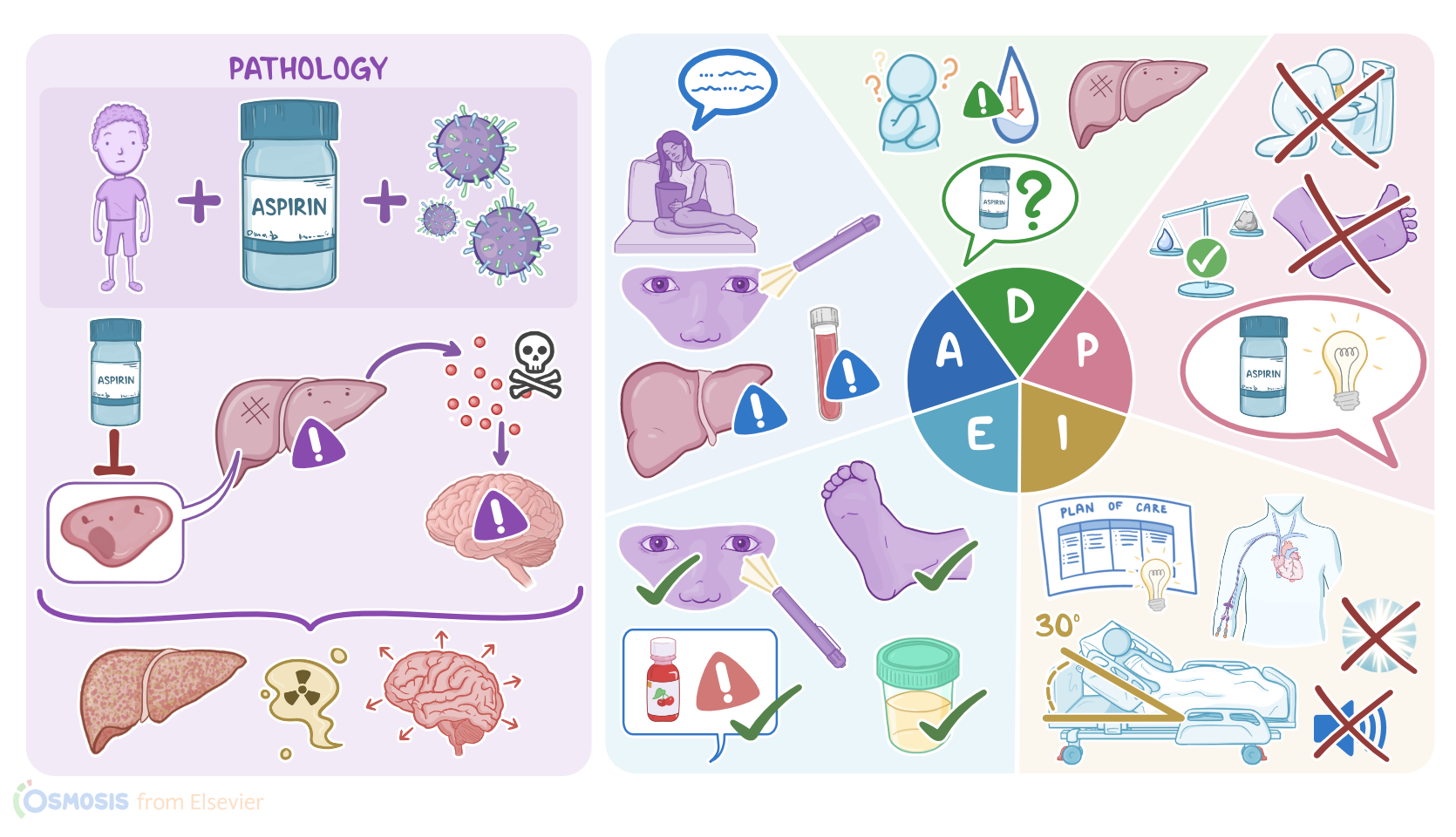
Reye syndrome is a rare but life-threatening condition that occurs in children younger than 18 years of age that take salicylate-containing medications like aspirin to treat a viral illness, especially influenza and varicella.
It is characterized by hepatic encephalopathy, where a liver dysfunction results in a buildup of toxic substances that causes brain dysfunction.
Now, the exact cause of Reye syndrome is not fully understood, but it’s thought that the use of salicylate medications may inhibit some important enzymes within the liver cells, or hepatocytes, leading to liver malfunction.
Now, hepatocytes have a variety of fundamental functions. First off, they play a key role in breaking down fatty acids to generate ATP, which is the main energy source for the body, via their metabolic powerhouses, the mitochondria.
Another important function of hepatocytes is the detoxification of harmful substances like medications, and byproducts of metabolism like ammonia, which is converted by hepatocytes into urea, to be excreted by the kidneys.
Hepatocytes are also involved in the production of most coagulation factors for blood clotting. Finally, hepatocytes are involved in the regulation of blood glucose.
In Reye syndrome, the malfunctioning hepatocytes are no longer able to perform their functions, such as producing ATP for energy, which leads to buildup of fatty acids in the liver, causing steatosis or fatty liver.
In addition, hepatocytes are no longer able to detoxify ammonia, resulting in hyperammonemia, or high ammonia levels in the blood, which is toxic to the brain.
This leads to encephalopathy, which presents with brain swelling and edema, which ultimately causes the intracranial pressure to rise.
Now, symptoms of Reye syndrome usually start after the onset of the viral illness treated with salicylates, and include severe and persistent vomiting, as well as declining brain function associated with lethargy, confusion, and impaired level of consciousness.
If not treated, Reye syndrome can put the client at risk of serious complications, including seizures and brain herniation. In addition, severe vomiting may put the client at risk of dehydration, acute renal failure, as well as aspiration pneumonia.
Clients may also be at risk of internal hemorrhage, and that's because the liver is unable to produce coagulation factors. Finally, Reye syndrome may lead to respiratory arrest, coma, and even death.
Now, diagnosis of Reye syndrome begins with history and clinical findings. On examination, clients may have hepatomegaly, or liver enlargement.
In addition, blood tests for Reye syndrome will be reflective of liver damage, typically showing hyperammonemia, as well as abnormal liver function tests.
These include increased levels of liver enzymes like aspartate aminotransferase, or AST, and alanine aminotransferase, or ALT. However, bilirubin levels are usually normal.
Another important thing to test is prothrombin time, or PT, which is the time it takes for the blood to coagulate, and is usually also elevated in Reye syndrome.
An arterial blood gas analysis can show metabolic acidosis, and a blood glucose level can show hypoglycemia, or less commonly, hyperglycemia. Also, a lumbar puncture can be performed to rule out other causes of encephalopathy, like meningitis and encephalitis.
Finally, imaging techniques like brain CT scan or MRI can show cerebral edema. Treatment of Reye syndrome involves careful monitoring, as well as supportive measures like intravenous fluids for dehydration, and dextrose-containing fluids to correct blood glucose levels.
Next, the cerebral edema and intracranial pressure can be reduced by giving osmotic diuretics, like mannitol or hypertonic saline. In addition, head elevation as well as induced hyperventilation with mechanical ventilation can help reduce fluid buildup in the brain.
To prevent Reye syndrome, it’s very important to avoid giving aspirin or other salicylates, such as bismuth subsalicylate, commonly known as Pepto-Bismol, to children and teenagers.
As Mrs. Jones and Gabriella arrive at the PICU, you assist them to get settled and begin your assessment. Gabriella is in the hospital bed and appears to be sleeping.
Mrs. Jones tells you how Gabriella became lethargic and has been vomiting with increased frequency and severity. She also states that the last time Gabriella urinated was 8 hours ago.