Age-related physiological changes: Nursing process (ADPIE)
Notes
| AGE-RELATED PHYSIOLOGIC CHANGES | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Matilda Nowell is a 78-year-old female client with a history of depression and osteoarthritis, who presents to the primary care clinic today with a report of frequent and prolonged episodes of constipation along with bloating and abdominal pain. Mrs. Nowell lives alone and has no family close by, and she struggles to afford nutritious food due to her limited income.
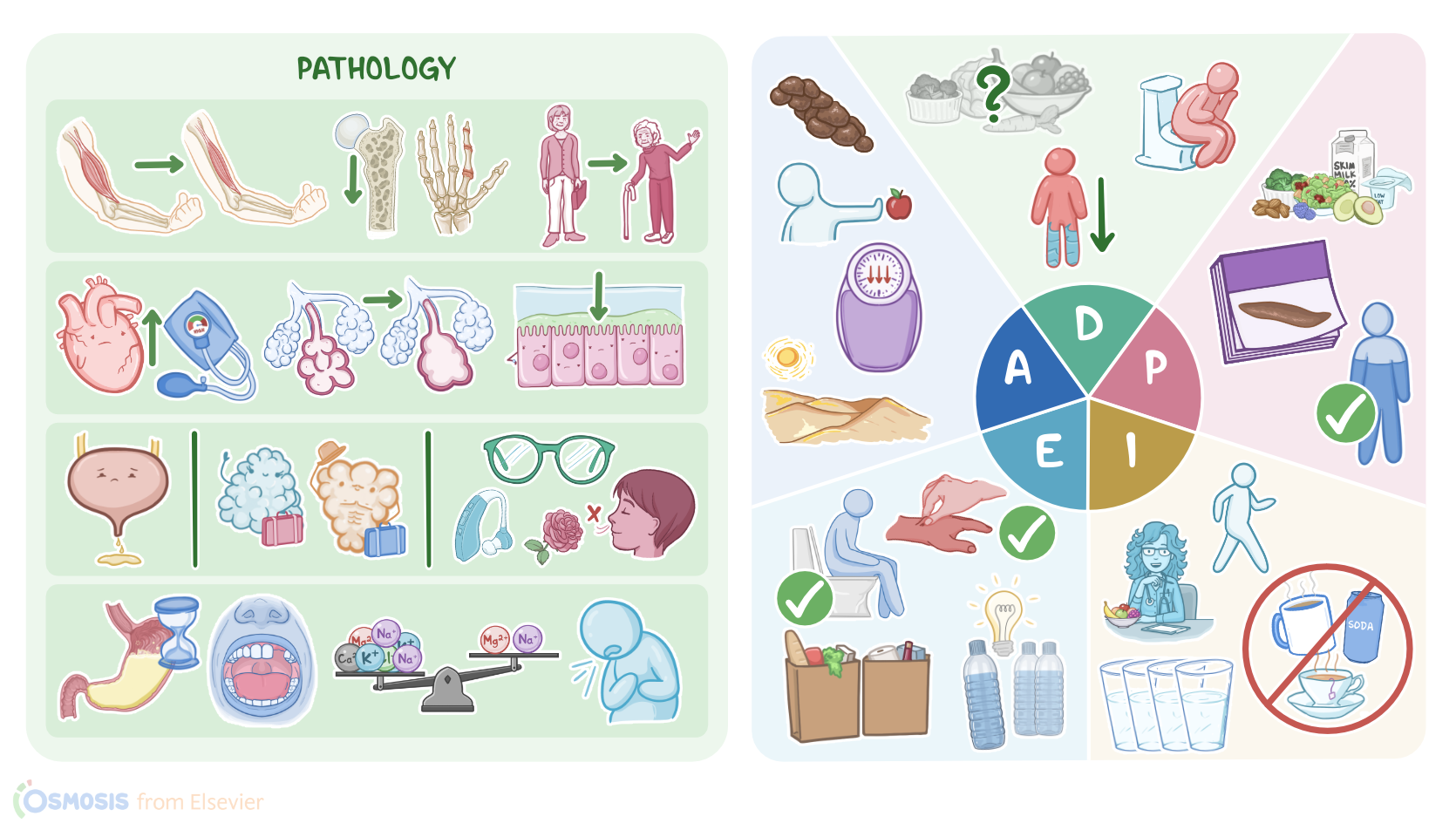
Age-related physiological changes include all changes that normally occur in the body over time with aging. First, let’s start with the integumentary system, which undergoes changes in collagen and elastin that eventually cause the skin to lose elasticity, become thinner, and develop wrinkles over time, while the hair becomes gray, thinner, and may fall out, which may lead to baldness. On the flip side, the muscular system atrophies over time, which often leads to a decrease in physical strength; while the skeletal system progressively loses bone mass and density, which typically leads to a gradual decrease in height, and can result in osteopenia or osteoporosis, therefore bones might break more easily, while joints may degenerate and develop arthritis.
Cardiovascular age-related changes generally involve progressive degeneration of the heart, while the valves and large arteries become stiffer, ultimately causing hypertension or decreased cardiac output upon exertion. On the other hand, changes of the respiratory system mainly involve the alveoli, which may lose their architecture and elasticity, which leads to a decreased lung capacity; in addition, there’s decreased mucociliary action and diminished cough reflex, so airway clearance is ultimately impaired.
The urinary system is affected by functional changes that decrease the filtration capacity of the kidneys; in addition, the bladder capacity is decreased, as there’s instability of the detrusor muscle and decreased sensation of bladder fullness, which combined result in urinary frequency or even incontinence; while the reproductive system is associated with gradually decreased production of sex hormones, and females become infertile after menopause. Also, over time, the sensory system can deteriorate, therefore older clients often present with decreased vision and hearing abilities, and some clients may also have impaired sense of smell and taste.
Finally, gastrointestinal age-related changes include dysphagia due to decreased esophageal motility, which can increase the risk of choking or aspiration; as well as delayed gastric emptying, slow gut transit time, and decreased absorption of nutrients. In addition, many clients may have altered dentition, such as missing or loose teeth, which makes it difficult to chew certain foods. Gastrointestinal age-related changes are among the most worrisome, as they can result in decreased food intake, ultimately leading to unintentional weight loss, malnutrition, constipation and fecal impaction; as well as severe dehydration and electrolyte imbalance. Now, these changes are most commonly caused by advanced age; poor nutrition and hydration; as well as side effects of certain medications like some antidepressants or opioids. Some risk factors include previous gastrointestinal conditions and sedentary lifestyle, which can further worsen gastrointestinal age-related changes.
Now, diagnosis of gastrointestinal age-related changes is primarily based on history and clinical features, as well as assessing their changes in height, weight, and BMI for a nutritional deficit. These clients typically present with signs of dehydration, like dry skin and mucous membranes, and poor skin turgor. In addition, they might complain of abdominal pain or bloating, and passing hard stools. Lab tests can be done to assess the complete blood count, which may often reveal anemia associated with abnormal transferrin levels. In addition, clients may present with decreased levels of nutrients, such as vitamins like folate and B12, and electrolytes like potassium, sodium, and chloride, as well as a decline in albumin levels. Additionally, imaging studies, like X-rays, can be performed to evaluate abdominal pain and bloating, and to detect fecal impaction.
Treatment of gastrointestinal age-related changes requires promoting adequate nutrition, hydration, and correction of electrolyte imbalance, as well as nutrient supplementation when necessary. Finally, clients who are taking medications associated with gastrointestinal side effects should be switched to an alternative medication.
You begin your assessment by asking Mrs. Nowell how she is feeling today. She informs you that she feels bloated and that her last bowel movement was a hard and lumpy stool 4 days ago. She denies blood in her stool and says she is still passing gas. She goes on to tell you that she doesn’t have an appetite and she’s not interested in preparing meals for herself. She says, “Food is so expensive these days.” When asked how much water she drinks each day, she says she is unsure. Her height is 5 feet, 7 inches; weight is 115 pounds, or 52.2 kg. Vital signs are tympanic temperature 98.2° F or 36.8°C; heart rate 76 and regular; respiratory rate 16 breaths per minute with clear breath sounds bilaterally; blood pressure 124/78 mmHg; SpO2 98% on room air; and pain 0/10. You note bowel sounds are hypoactive in all four quadrants. You continue your assessment by noticing that skin turgor is decreased and her mucous membranes are dry.
Key Takeaways
With aging, several physiological changes take place in our bodies. These include the reduction of cardiac output, an increase in the blood pressure as arteriosclerosis develops, a decrease in the vital capacity of our lungs, slowing down of alveolar gas exchange, a decline in our creatinine clearance, and so on. When providing nursing care to older people, the ADPIE framework can be used to help nurses systematically assess and address these changes:
A: Assessment: taking a complete health history and performing a physical exam to identify any changes since the last visit; D: Diagnosis: identifying any specific problems or concerns that need to be addressed; P: Planning: creating a care plan tailored to the individual's needs; I: Implementation: providing care based on the plan; and E: Evaluation: assessing how well the plan is working and making any necessary adjustments.
Sources
- "Diagnosing the Diagnostic and Statistical Manual of Mental Disorders: Fifth Edition" Routledge (2019)
- "First Aid for the USMLE Step 1 2022, 32E" McGraw-Hill Education (2022)
- "Saunders Comprehensive Review for the NCLEX-RN Examination" Elsevier (2022)
- "Critical care nursing: Diagnosis and management " Elsevier (2022)
- "Harrison's Principles of Internal Medicine, Twenty-First Edition (Vol.1 & Vol.2)" McGraw-Hill Education / Medical (2022)
- "Physical activity and cardiovascular aging: Physiological and molecular insights" Experimental Gerontology (2018)
- "Regulation of inflammation as an anti‐aging intervention" The FEBS Journal (2019)