Acute kidney injury (AKI): Nursing process (ADPIE)
4,573views
Acute kidney injury (AKI): Nursing process (ADPIE)
Synthesis Of Nursing Practice
Synthesis Of Nursing Practice
Notes
| ACUTE KIDNEY INJURY (AKI) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| CLINICAL FEATURES AND COMPLICATIONS |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION | ||
Transcript
You are assigned to take care for Maurice Jones, a 58-year-old Black male, who sustained a back injury several weeks ago while cleaning out his garage, and since then he’s been taking ibuprofen three to four times each day for pain. Mr. Jones has a history of hypertension for which he takes the angiotensin II receptor blocker, or ARB, losartan, though he says sometimes he forgets to take it. He also takes the proton pump inhibitor, or PPI, omeprazole, for gastrointestinal reflux disease, or GERD. He presented to his primary care provider, or PCP, with fatigue, headache, lower extremity edema, and decreased urine output.
His vital signs were oral temperature 99.0 F or 37 C, heart rate 98 beats per minute, respiratory rate 20 breaths per minute and blood pressure 148/96mmHg. Labs were ordered which showed BUN 28 mg/dL, creatinine 2.4 mg/dL, sodium 124 mEq/L, and potassium 5.3 mEq/L. Arterial blood gas analysis revealed pH 7.25, PCO2 32, PO2 85, HCO3 30. Urine specific gravity is 1.010. Mr. Jones was admitted to the medical unit with a diagnosis of acute kidney injury, or AKI.
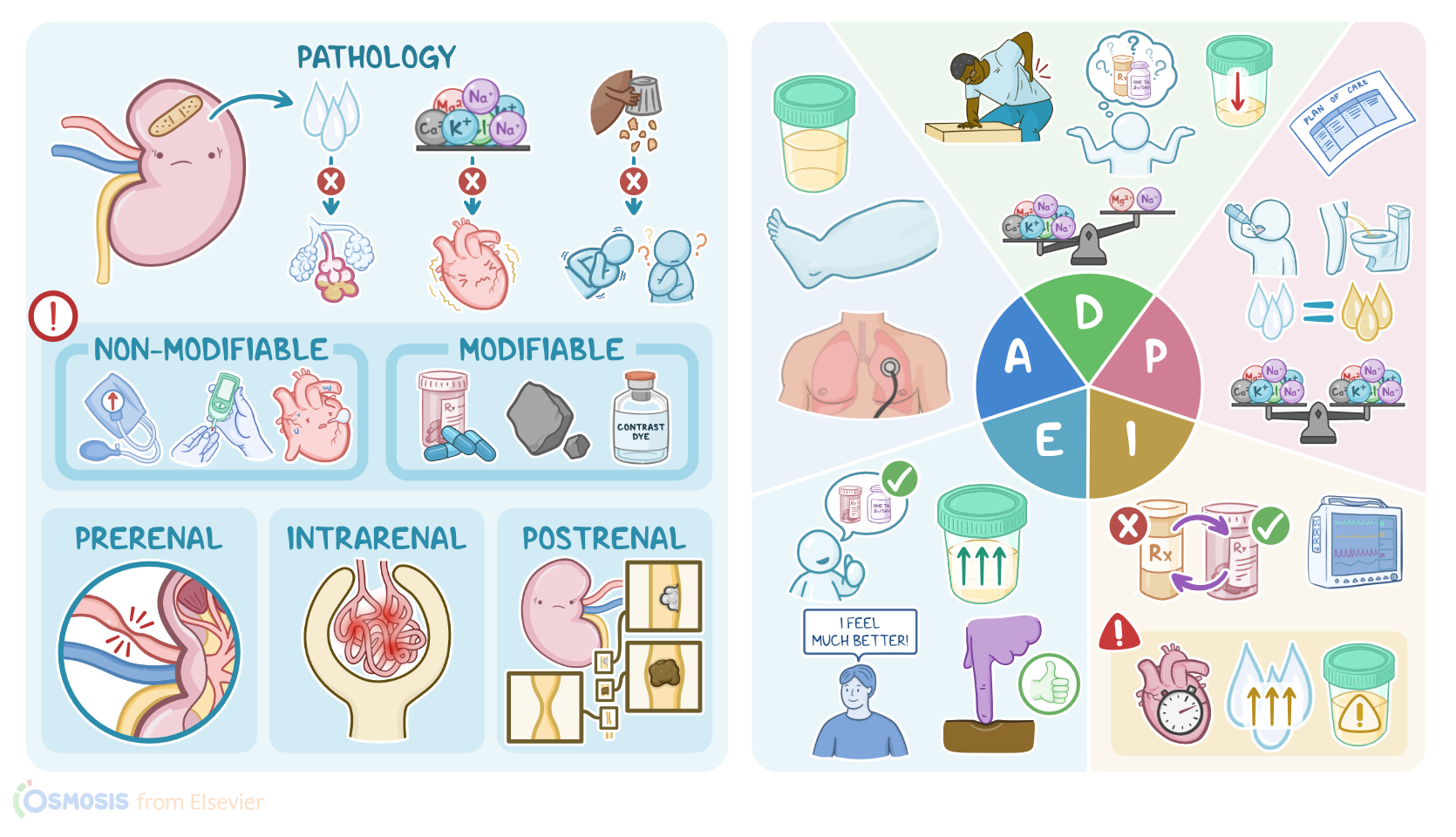
Acute kidney injury, or AKI for short, refers to a sudden decrease in kidney function over hours or days. As a result, the kidney’s ability to manage fluid, electrolyte, and acid-base balance is impaired, and there’s decreased excretion of waste products, such as urea and creatinine, which build up in the blood.
There are some factors that can put an individual at risk for AKI. Unfortunately, many of them are non-modifiable factors that decrease kidney function over time, such as advanced age, diabetes mellitus, autoimmune diseases, certain cancers, uncontrolled hypertension, and heart, liver, or kidney disease. Some modifiable risk factors include exposure to nephrotoxic agents, such as certain antibiotics, heavy metals, or chemotherapy or being exposed to iodinated IV contrast dye during radiology procedures.
Now, the causes of AKI can be classified into prerenal, intrarenal, and postrenal. In prerenal AKI there is no physical problem with the kidneys themselves, but the problem is caused by decreased blood flow to the kidneys. This can happen when there’s a severe loss of body fluid due to problems like hemorrhage, burns, or ascites. Other common causes involve decreased cardiac output, like with heart failure, myocardial infarction, or shock. Intrarenal AKI occurs due to damage to the kidney itself. Some common causes include inflammatory problems like glomerulonephritis and damage done by toxins, or prolonged ischemic injury. Finally, postrenal AKI occurs due to decreased outflow of urine from the kidneys. This can be a result of something compressing the ureter, like tumors, strictures, or an enlarged prostate, or from an obstruction caused by kidney stones lodged in the ureters.
AKI generally progresses through three phases, oliguric, diuretic, and recovery. Often the first sign of AKI is decreased urine output, which can lead to fluid overload, peripheral edema, and weight gain, as well as hypertension. A bounding pulse and distended neck veins could also be present. Over time, this can lead to complications like pulmonary edema, which causes dyspnea and tissue hypoxia.
Next, electrolytes can also become imbalanced since the damaged kidneys aren’t able to excrete them effectively from the body. Those who develop hyperkalemia may experience muscle weakness and dangerous cardiac arrhythmias. In addition, phosphate retention leads to hyperphosphatemia, which can ultimately lead to hypocalcemia, resulting in tetany, which are involuntary muscle cramps. As uremic waste products build up in blood, the client can experience symptoms like anorexia or appetite loss, nausea, and vomiting, as well as uremic encephalopathy, which is initially characterized by confusion and lethargy, and may progress to seizures and even coma. Finally, if AKI is not treated, it may progress to permanent kidney damage or end-stage renal disease, and death.
The main diagnostic studies used for AKI include standard laboratory tests that can show abnormal electrolyte levels like hyperkalemia, hyperphosphatemia, and hypocalcemia. Blood urea nitrogen, or BUN, and creatinine will also be elevated. A blood gas analysis can show metabolic acidosis. In addition, urinalysis can reveal proteinuria, hematuria, and casts. Finally, imaging techniques like an ultrasound or CT scan can assess renal blood flow and allow identification of an underlying cause.
Key Takeaways
Acute kidney injury (AKI) is a sudden, potentially reversible decline in renal function. AKI results in the accumulation of water, nitrogenous wastes, sodium, and other metabolic wastes in the body, and can also lead to electrolyte imbalances. Common causes include dehydration, sepsis, and some drug therapy.
AKI often presents with reduced urine output, but there can be other signs such as edema, and those associated with the accumulation of metabolic wastes such as anorexia, seizures, and altered mental status. The nursing process for AKI begins with the assessment and identification of patients at risk for developing the condition. Once AKI is diagnosed, nurses work with other health care providers to implement therapies aimed at preventing progression and maximizing patient outcomes. If AKI is left untreated, it can lead to chronic kidney disease (CKD).
Sources
- "Diagnosing the Diagnostic and Statistical Manual of Mental Disorders: Fifth Edition" Routledge (2019)
- "Saunders Comprehensive Review for the NCLEX-RN Examination" Elsevier (2022)
- "Critical care nursing: Diagnosis and management (9th ed)" Elsevier (2022)
- "Harrison’s principles of internal medicine" Mcgraw Hill (2022)
- "Sepsis associated acute kidney injury" BMJ (2019)
- "Acute kidney injury in the critically ill: an updated review on pathophysiology and management" Intensive Care Medicine (2021)
- "Robbins Basic Pathology" Elsevier (2017)