Brachial plexus injury: Nursing
Brachial plexus injury: Nursing
Newborn
Newborn
Notes
| BRACHIAL PLEXUS INJURY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Brachial plexus injury describes damage to the brachial plexus, which is a network of nerves that supply motor and sensory innervation to the upper limbs.
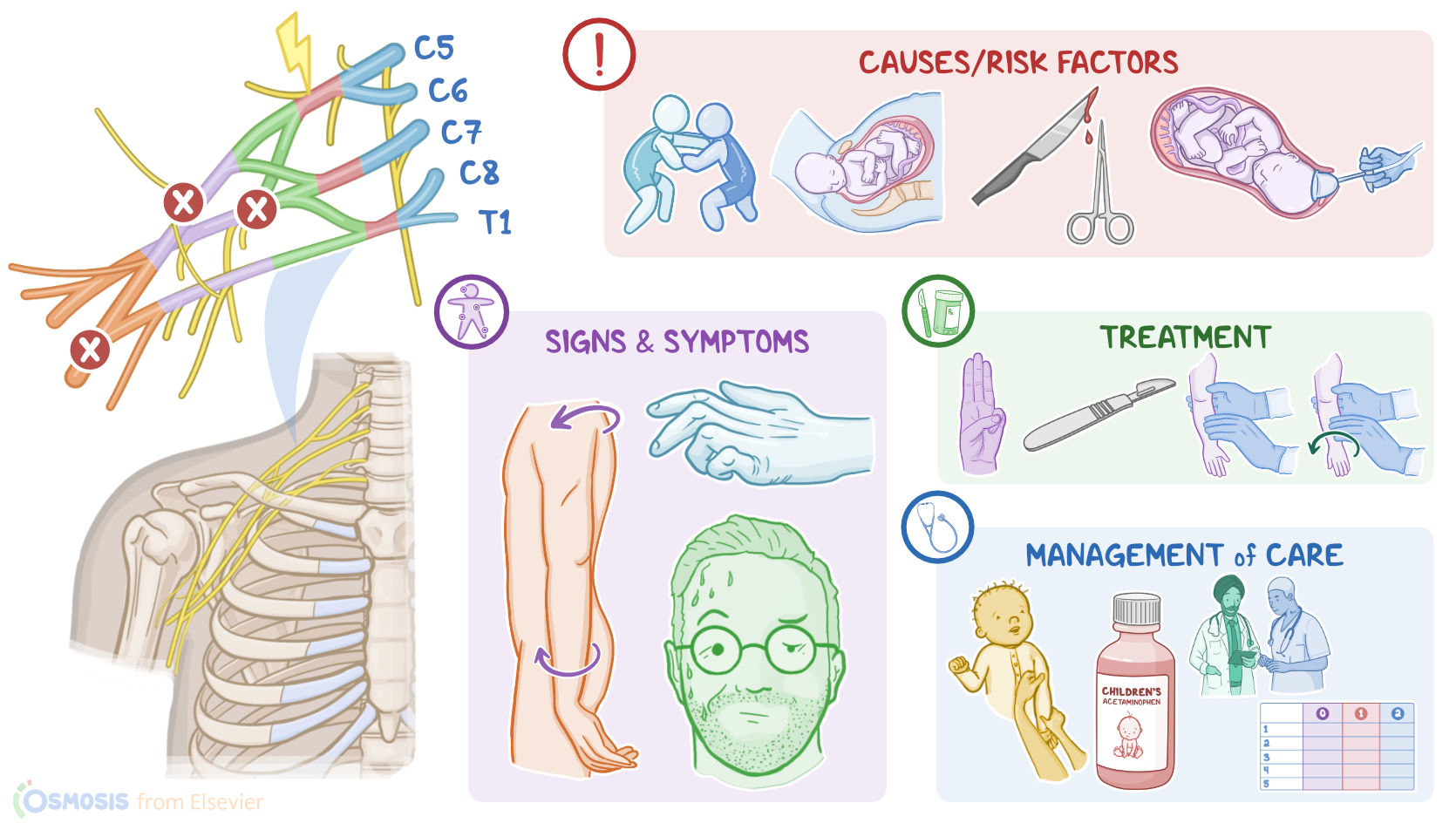
First, let’s go over some anatomy and physiology. The brachial plexus is divided into roots, trunks, divisions, cords, and branches. The roots are the ventral rami coming from spinal nerves C5 to T1. These roots combine to form the next part of the brachial plexus, called the superior or upper, middle, and inferior or lower trunks.
Then, these trunks give off divisions, which in turn recombine to form the lateral, posterior, and medial cords. Finally, these cords give off branches, which give rise to the musculocutaneous, axillary, radial, median, and ulnar nerves, which supply motor and sensory innervation to different areas of the upper limb.
The musculocutaneous nerve gives motor innervation to the muscles of the anterior arm, as well as sensory innervation to the lateral side of the forearm. On the other hand, the axillary nerve carries motor information to the teres minor and deltoid muscles. It also carries sensory information from the shoulder joint, and the skin covering the inferior portion of the deltoid.
The radial nerve gives sensory and motor innervation to the posterior arm and forearm. In the hand, it only supplies sensory innervation on the dorsal side. Here, it innervates the lateral hand, the thumb, and the proximal 2nd to 4th digits.
Next, the median nerve provides motor innervation to most muscles of the anterior forearm. In the hand, it innervates the thenar muscles, which act on the thumb, and the lateral lumbrical muscles of the other digits. The median nerve also carries sensory information from the skin of the hand; on the palmar side, it innervates the lateral 3 ½ digits and the adjacent palm. On the dorsal side, it innervates the distal aspects of the lateral 3 ½ digits.
Finally, the ulnar nerve carries motor information to the flexor carpi ulnaris, and the ulnar half of flexor digitorum profundus in the forearm. In the hand, it innervates most of the intrinsic muscles, except for a couple that are innervated by the median nerve.
Just like the median and radial nerves, the ulnar nerve also carries sensory information from the skin of the hand; on the palmar side, it supplies the medial 1 ½ digits and the adjacent palm. On the dorsal side, it also innervates the medial 1 ½ digits and the adjacent skin of the hand.
Now, the most common cause of brachial plexus injury is birth trauma from traction on the arm when the infant is passing through the birth canal. Other causes of brachial plexus injury include trauma like sport injuries, falls, surgical procedures, or stab wounds. Lastly, Pancoast tumors, which are tumors that develop at the lung’s apex, can compress the brachial plexus.
Risk factors for brachial plexus injury include large babies; prolonged labor; precipitous labor, which is labor that lasts less than three hours, resulting in a rapid delivery; and shoulder dystocia, which can happen when one of the baby’s shoulders get stuck during delivery; as well as the use of forceps or vacuum to extract the baby during delivery; and breech position.
Now, the pathology of brachial plexus injury starts with a stretch, tear or hemorrhage of one or more nerves arising from the brachial plexus. Depending on the injured nerve and the location of the injury, the nerve won’t be able to transmit motor signals or receive sensory signals from the innervated areas, which causes impaired sensation or movement in the affected limb. Sometimes, there can be paralysis of the affected limb, which is called palsy.
The two main palsies linked to brachial plexus injury include Erb and Klumpke. In Erb palsy, there’s an injury to the upper trunk of the brachial plexus, which is typically caused by an increase in the angle between the neck and the shoulder. This causes loss of sensation in the upper arm, in addition to paralysis to the deltoid, biceps, and brachialis muscles. On the other hand, Klumpke palsy happens with an injury to the lower trunk of the brachial plexus, which is typically caused by excessive upward pulling of the upper limb. This causes paralysis of the intrinsic muscles of the hand.
The clinical manifestations of brachial plexus injury typically include impaired sensation, movement, or strength of the affected upper limb, or, in some cases, palsy. With Erb palsy, the main clinical finding is the so-called waiter’s tip sign, in which there’s internal rotation at the shoulder joint, adduction of the upper limb, extension and pronation of the forearm, in addition to flexion of the wrist and extension of the fingers.
On the other hand, Klumpke palsy causes the claw hand sign, in which there’s supination of the forearm, extension of the wrist, and flexion of the fingers. Klumpke palsy can also be associated with Horner syndrome, which affects the sympathetic nerves of the T1 nerve root. Clients with Horner’s syndrome typically present with unilateral drooping eyelids, called ptosis; smaller pupils, called miosis; and decreased sweat production in the face, called anhidrosis.
Finally, both Erb and Klumpke palsies can cause loss of reflexes, including the Moro reflex in newborns, as well as the biceps, and brachioradialis reflexes in both newborns and adults.