Osteomyelitis: Nursing
1,633views
Notes
| OSTEOMYELITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
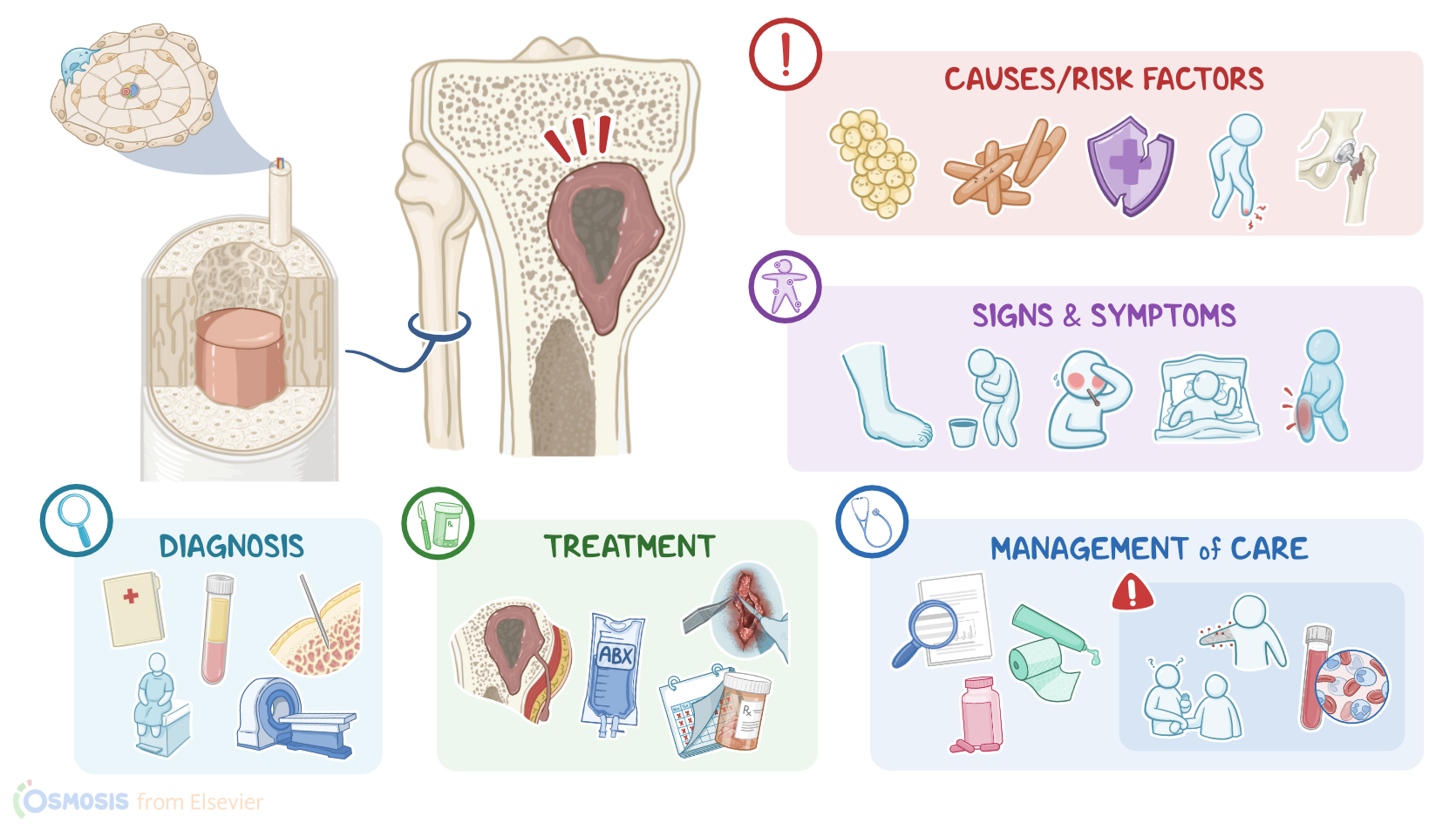
Osteomyelitis is an inflammation of the bone and its associated structures, and it typically results from an infection. Osteomyelitis can be acute, when symptoms last up to one month; or chronic, when symptoms last more than one month.
Now, normally, the bones’ surface is covered by a dense layer of connective tissue called the periosteum, and it's where the muscles, tendons, and ligaments are attached. Beneath the periosteum, there’s a dense external layer called compact bone. This consists of many tiny cylinders known as osteons, which form the structural and functional units of bones. Each osteon is composed of concentric layers of collagen and hydroxyapatite surrounding a central canal called the Haversian canal, which contains the nerves and blood vessels that supply the osteon. In the center of the bone, there’s the medullary canal, a hollow space lined by a honeycomb- looking structure called the spongy or cancellous bone. This is made of crosslinking tiny roads called trabeculae, which make bones resistant to mechanical stress so that they can bear weights without caving in. The spaces in the spongy bone are occupied by the bone marrow, which is the site of blood cell production.
Now, the most common cause of osteomyelitis is an infection with Staphylococcus aureus, which is a round-shaped bacterium that normally lives on the skin. Other bacteria that can cause osteomyelitis include Mycobacterium tuberculosis, Pseudomonas aeruginosa, Streptococcus spp., Salmonella spp., and Pasteurella spp. Less commonly, osteomyelitis might also be caused by viruses, parasites, and fungi.
Risk factors for osteomyelitis can be grouped into local and systemic ones. Local risk factors include trauma and open wounds. Systemic risk factors, on the other hand, include having a weak immune system, which can be because of an HIV infection, as well as poor circulation, which could be due to uncontrolled diabetes or peripheral vascular disease. Bacterial infections at other sites of the body, including the ears, tonsils, teeth, sinuses, lungs, and genitourinary tract, can also increase the risk of developing osteomyelitis. Lastly, IV drug use, periodontal disease, and having an indwelling central catheter or prosthetic joint increase the risk of osteomyelitis.
Now, the pathology of osteomyelitis starts with the direct or indirect invasion of bones by the causative pathogen. Direct invasion is associated with trauma or surgery. For example, in an open fracture after an accident, the bone may get exposed to the outside environment, coming in direct contact with bacteria. In contrast, indirect invasion happens either from a distant infection through the bloodstream, called hematogenous spread, or from a nearby infection, like cellulitis, which is an infection of the dermis layer of the skin, and this is known as contiguous spread.
Now, once the pathogens reach the bone by any of these routes, they start to proliferate and initiate an inflammatory response, which causes local destruction of the bone. This is the acute phase of the disease and typically resolves within a period of weeks. However, in some cases, the process turns into chronic osteomyelitis, lasting months to years. In that situation, the affected bone sometimes becomes necrotic and separates from the healthy part of the bone, and that’s called a sequestrum. Occasionally, in both acute and chronic osteomyelitis the inflammation may involve the periosteum, lifting it up away from the compact bone. The infection can also spread further to involve a nearby joint, particularly the knee or hip joint, as well as overlying muscle, skin, and even get into blood, causing bacteremia and sepsis. Other complications include septic arthritis or pathologic fractures at the site of infection. Osteomyelitis can affect any bone, but it's particularly worrisome when it involves bones of the skull or the spine, where it could result in spinal cord compression, meningitis, or brain abscess.
Now, signs and symptoms of osteomyelitis can be local and include bone pain, redness, swelling, warmth, in addition to restricted movement around the site of infection. On the other hand, systemic signs and symptoms include fever, malaise, nausea, restlessness, and night sweats or chills.
The diagnosis of osteomyelitis starts with the client's history and physical assessment, followed by laboratory tests. These include a complete blood count or CBC which shows an increase in white blood cells, as well as an elevated erythrocyte sedimentation rate or ESR and C-reactive protein or CRP. In addition, imaging tests, such as an X-ray, CT scan, MRI, and radionuclide bone scans can show thickening of the cortical bone and periosteum as well as elevation of the periosteum. Other findings may include loss of the normal trabecular architecture of the bone or osteopenia, which refers to loss of bone mass. When possible, a bone biopsy is also taken or histopathologic examination and culture to confirm the diagnosis and identify the pathogen responsible for the infection.
Treatment of acute osteomyelitis starts with intravenous administration of antibiotics, followed by surgical debridement, if needed. Irrigation of the area with antibiotics can also be done. In addition, acrylic bead chains containing antibiotics can be implanted into the infected bone to eradicate the infection.
On the other hand, the treatment of chronic osteomyelitis includes incision and drainage, wound debridement, and sequestrectomy, which is the surgical removal of dead tissue. This is followed by extended antibiotics therapy and hyperbaric oxygen therapy, which has been shown to enhance bone and soft tissue healing. Finally, in severe cases of chronic osteomyelitis, amputation of the affected limb, along with a bone graft might be needed.
Alright, let’s look at the nursing care you’ll provide for a client with osteomyelitis. Your priority goals of care are to eradicate the infection and monitor for complications.