Reye syndrome: Nursing process (ADPIE)
Client Report0:00–0:44
Gabriella Jones is a six-year-old girl who was brought to the emergency department by her mother. Mrs.
Jones states that for the past 24 hours Gabriella has become increasingly lethargic with rapid breathing and has been vomiting for the past two days.
Mrs. Jones adds that about one week ago, Gabriella had influenza and her pediatrician recommended acetaminophen if Gabriella developed a fever.
Mrs. Jones didn’t have any acetaminophen on hand, so she gave Gabriella two doses of aspirin instead after Gabriella developed a fever.
Gabriella is admitted to the pediatric intensive care unit, or PICU, with a probable diagnosis of Reye syndrome. Reye syndrome is a rare but life-threatening condition that occurs in children younger than 18 years of age that take salicylate-containing medications like aspirin to treat a viral illness, especially influenza and varicella.
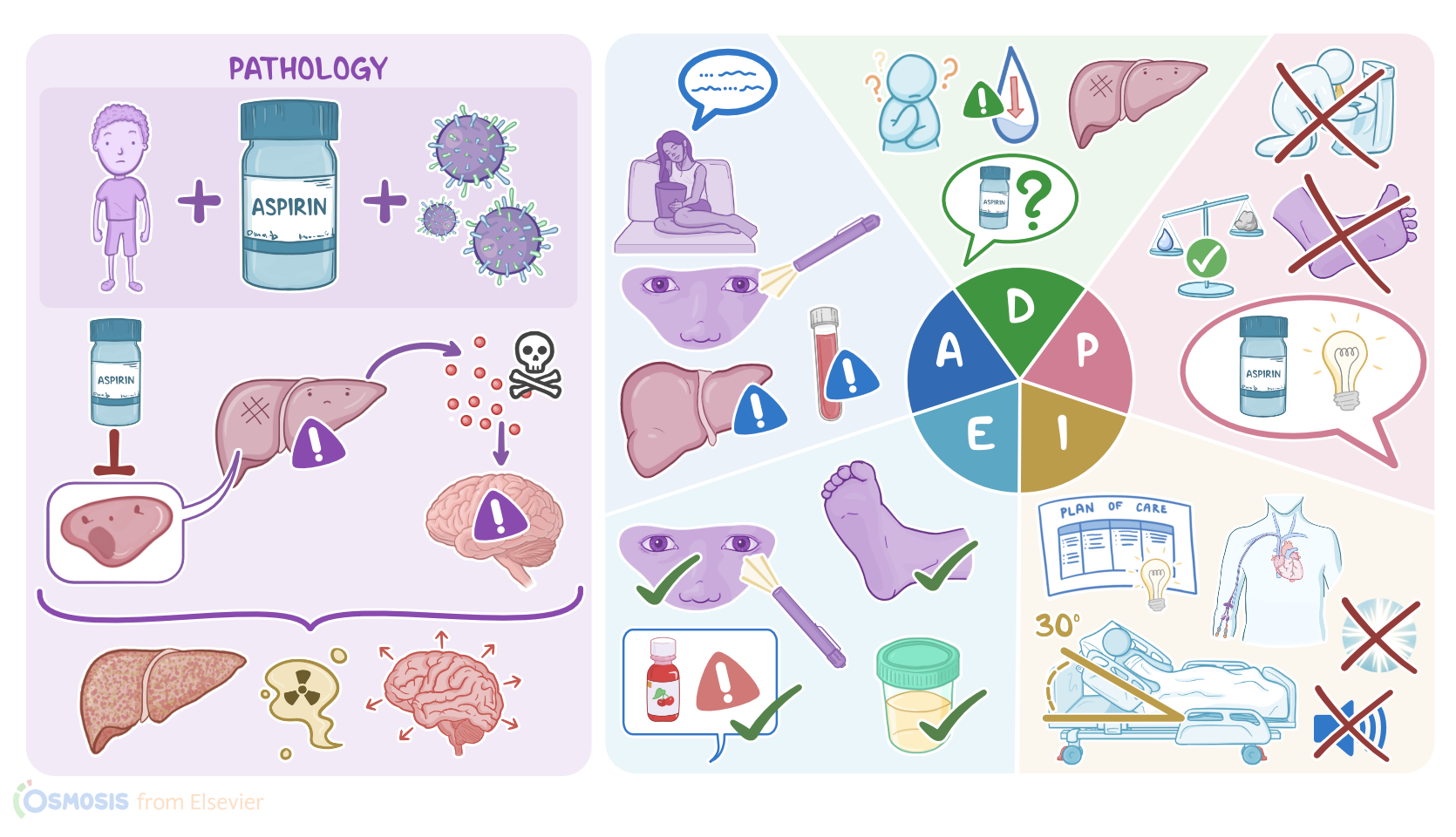
Pathology0:44–5:03
It is characterized by hepatic encephalopathy, where a liver dysfunction results in a buildup of toxic substances that causes brain dysfunction.
Now, the exact cause of Reye syndrome is not fully understood, but it’s thought that the use of salicylate medications may inhibit some important enzymes within the liver cells, or hepatocytes, leading to liver malfunction.Now, hepatocytes have a variety of fundamental functions.
First off, they play a key role in breaking down fatty acids to generate ATP, which is the main energy source for the body, via their metabolic powerhouses, the mitochondria.
Another important function of hepatocytes is the detoxification of harmful substances like medications, and byproducts of metabolism like ammonia, which is converted by hepatocytes into urea, to be excreted by the kidneys.
Hepatocytes are also involved in the production of most coagulation factors for blood clotting. Finally, hepatocytes are involved in the regulation of blood glucose.In Reye syndrome, the malfunctioning hepatocytes are no longer able to perform their functions, such as producing ATP for energy, which leads to buildup of fatty acids in the liver, causing steatosis or fatty liver.
In addition, hepatocytes are no longer able to detoxify ammonia, resulting in hyperammonemia, or high ammonia levels in the blood, which is toxic to the brain.This leads to encephalopathy, which presents with brain swelling and edema, which ultimately causes the intracranial pressure to rise.Now, symptoms of Reye syndrome usually start after the onset of the viral illness treated with salicylates, and include severe and persistent vomiting, as well as declining brain function associated with lethargy, confusion, and impaired level of consciousness.If not treated, Reye syndrome can put the client at risk of serious complications, including seizures and brain herniation.
In addition, severe vomiting may put the client at risk of dehydration, acute renal failure, as well as aspiration pneumonia.
Clients may also be at risk of internal hemorrhage, and that's because the liver is unable to produce coagulation factors.
Finally, Reye syndrome may lead to respiratory arrest, coma, and even death.Now, diagnosis of Reye syndrome begins with history and clinical findings.
On examination, clients may have hepatomegaly, or liver enlargement. In addition, blood tests for Reye syndrome will be reflective of liver damage, typically showing hyperammonemia, as well as abnormal liver function tests.
These include increased levels of liver enzymes like aspartate aminotransferase, or AST, and alanine aminotransferase, or ALT.
However, bilirubin levels are usually normal. Another important thing to test is prothrombin time, or PT, which is the time it takes for the blood to coagulate, and is usually also elevated in Reye syndrome.
An arterial blood gas analysis can show metabolic acidosis, and a blood glucose level can show hypoglycemia, or less commonly, hyperglycemia.
Also, a lumbar puncture can be performed to rule out other causes of encephalopathy, like meningitis and encephalitis. Finally, imaging techniques like brain CT scan or MRI can show cerebral edema.
Treatment of Reye syndrome involves careful monitoring, as well as supportive measures like intravenous fluids for dehydration, and dextrose-containing fluids to correct blood glucose levels.
Next, the cerebral edema and intracranial pressure can be reduced by giving osmotic diuretics, like mannitol or hypertonic saline.
In addition, head elevation as well as induced hyperventilation with mechanical ventilation can help reduce fluid buildup in the brain.
To prevent Reye syndrome, it’s very important to avoid giving aspirin or other salicylates, such as bismuth subsalicylate, commonly known as Pepto-Bismol, to children and teenagers.
Assessment5:03–7:14
As Mrs. Jones and Gabriella arrive at the PICU, you assist them to get settled and begin your assessment.
Gabriella is in the hospital bed and appears to be sleeping. Mrs.
Jones tells you how Gabriella became lethargic and has been vomiting with increased frequency and severity. She also states that the last time Gabriella urinated was 8 hours ago.
You gently try to wake her and she opens her eyes and begins to mumble incoherently. She is unable to state her name or her age.
Her pupils are slightly dilated and have a sluggish response to light. She withdraws her hand from a painful stimulus.
Her reflexes are hyperactive and the Babinski sign is positive. While palpating her abdomen, you notice that her liver feels enlarged.
Her vital signs are: temporal temperature 98.7 F or 37 C, heart rate 120 beats per minute, respiratory rate 35 breaths per minute, blood pressure 85/55 mmHg, SpO2 97% on room air, and pain 4/10 using the FLACC scale.
Next, you note these laboratory results: AST 150 U/L, ALT 98 U/L, total bilirubin 0.5 mg/dL, ammonia 165 mcg/dL, blood glucose 80 mg/dL, BUN 25 mg/dL, creatinine 0.7 mg/dL, PT 25 seconds, and platelet count 120,000/mm3.
Arterial blood gas analysis results are pH 7.36, PaO2 80mmHg, PaCO2 32mmHg and bicarbonate 21mEq/L. A brain CT scan detected cerebral edema.
You document your assessment findings and continue to monitor Gabriella for indications that her condition is worsening, including the presence of seizures, bleeding, and mental status changes.After performing your assessment, you formulate your nursing diagnoses for Gabriella, which include: acute confusion related to increased intracranial pressure and increased ammonia levels; deficient fluid volume related to vomiting; risk for hemorrhage related to liver dysfunction; and for Mrs.
Jones, deficient knowledge related to use of antipyretics.Now it is time to plan goals for Gabriella and Mrs. Jones.
Diagnosis7:14–7:34
By the end of your shift, Gabriella’s orientation to her environment will be improved, her neurological assessments will normalize, and there will be no signs of bleeding.
By discharge, Gabriella will have no more episodes of vomiting, normal fluid balance will be restored, and Mrs. Jones will verbalize understanding of the safe use of antipyretics.
Planning7:34–7:58
Next, you begin implementing interventions for Gabriella. First, you implement measures to reduce intracranial pressure, which include keeping the bed at a 30 degree angle, maintaining the head and neck in a neutral, midline position, reducing environmental stimuli, and carefully monitoring fluid balance.
A peripherally inserted central catheter, or PICC line, is inserted in order to administer the anti-hyperammonemic medication sodium phenylacetate/sodium benzoate, as well as the serotonin antagonist ondansetron.
Implementation7:58–9:05
Your hourly checks include monitoring vital signs, fluid intake and output, neurologic status, and the presence of bleeding.
You also monitor laboratory values as needed. Next, you explain to Mrs.
Jones about safe use of over-the-counter medications, especially antipyretics, and remind her to always read and take note of directions and warnings on medication labels.
You emphasize the importance of consulting a physician or pharmacist if she is unsure about the appropriateness of a medication for her child.
It’s almost time for shift change, so you evaluate how Gabriella is doing so far. Gabriella is still lethargic, however she can tell you her name and how old she is.
Evaluation9:05–10:35
Gabriella had one episode of vomiting and she is producing an adequate amount of clear, yellow urine. Her most recent labs include BUN 20 mg/dL, creatinine 0.6 mg/dL, glucose 100 mg/dL, and PT 15 seconds.
Her latest arterial blood gas analysis results are pH 7.38, PaO2 80 mmHg, PaCO2 36 mmHg and bicarbonate 22 mEq/L. Gabriella’s vital signs are temporal temperature 98.6 F or 37 C, heart rate 110 beats per minute and regular, respiratory rate 22 breaths per minute and regular, blood pressure 94/56mmHg, SpO2 97% on room air, and pain is 0/10.
Mrs. Jones tells you she will keep acetaminophen on hand for the next time Gabriella develops a fever and that she understands the importance of always carefully reading medication labels.
Alright, as a quick recap … Gabriella Jones is a 6-year-old girl who was brought to the emergency department by her mother with complaints of vomiting and lethargy after receiving aspirin during a viral infection.
Your assessment findings included an altered mental status, abnormal pupillary responses, elevated liver function tests and ammonia levels.
Your nursing diagnosis for Gabriella included acute confusion; deficient fluid volume; risk for hemorrhage; and deficient knowledge for Mrs.
Jones. You planned goals to improve Gabriella’s neurological status and fluid balance and to teach Mrs.
Summary10:35–11:31
Jones about the safe use of antipyretics. Your interventions focused on reducing ICP, correcting fluid and metabolic imbalances, monitoring for complications, and providing Mrs.
Jones with education about the use of antipyretics. You continue to evaluate Gabriella before giving your handoff report to the oncoming nurse.
for Gabriella's included, acute confusion deficient fluid volume risk for Hemorrhage, and deficient knowledge for mrs. Jones, you plan goals to improve Gabriella's neurological status and fluid.
Balance teacher, mrs. Jones about the safe use of antipyretics.
Your interventions focused on reducing ICP correcting fluid, and metabolic imbalances monitoring for complications and providing message with education about the use of antipyretics.
You continue to evaluate Gabriella before, giving your hand off report to the oncoming nurse.
| REYE SYNDROME | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
No notes for this video yet
Try adding a note below