Seizure disorder: Nursing process (ADPIE)
2,249views
Seizure disorder: Nursing process (ADPIE)
FINAL
FINAL
Notes
| SEIZURE DISORDER | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Francisco Bernard is an 18-year-old male client who was brought to the emergency department, or ED, after his father witnessed him suddenly go rigid, lose consciousness, and fall to the floor.
His arms and legs immediately began to jerk rapidly, then slow and eventually stop. Afterwards, Francisco was confused and lethargic with no memory of what happened.
Upon arrival in the ED Francisco was awake but disoriented. He was transferred to the neurological unit where he was diagnosed with epilepsy. A seizure is a sudden event that occurs due to abnormal, excessive, and synchronous firing from neurons in the brain.
This manifests as a change in the client's level of consciousness, body movements, sensation, or autonomic functions, that usually last for a few seconds or minutes.
Seizures can be triggered by stress, tiredness, and lack of sleep. High fever, especially in young children, as well as infections like meningitis, encephalitis, or brain abscess, can also result in seizures.
Also, withdrawal of certain substances like alcohol, cocaine, benzodiazepines and barbiturates may cause seizures. During pregnancy, seizures can be provoked by eclampsia, which occurs in the setting of high blood pressure.
Now, epilepsy is when a client has two or more seizures separated by at least 24 hours. A very important risk factor for epilepsy is family history.
Epilepsy can also be caused by brain damage due to traumatic brain injury or stroke, as well as brain tumors. Other causes include congenital diseases like Sturge-Weber Syndrome, metabolic disorders like phenylketonuria, as well as neurodegenerative diseases such as Alzheimer’s disease.
In many cases, however, the cause of epilepsy is unknown.Right before having a seizure, clients may experience neurological symptoms called auras, which present with subtle muscle movements called automatisms, such as chewing, lip smacking, or rapid blinking.
Some clients may also report smelling unusual odors like kerosene, a rising sensation in the abdomen, an unusual taste, or even feelings of fear or déjà vu.
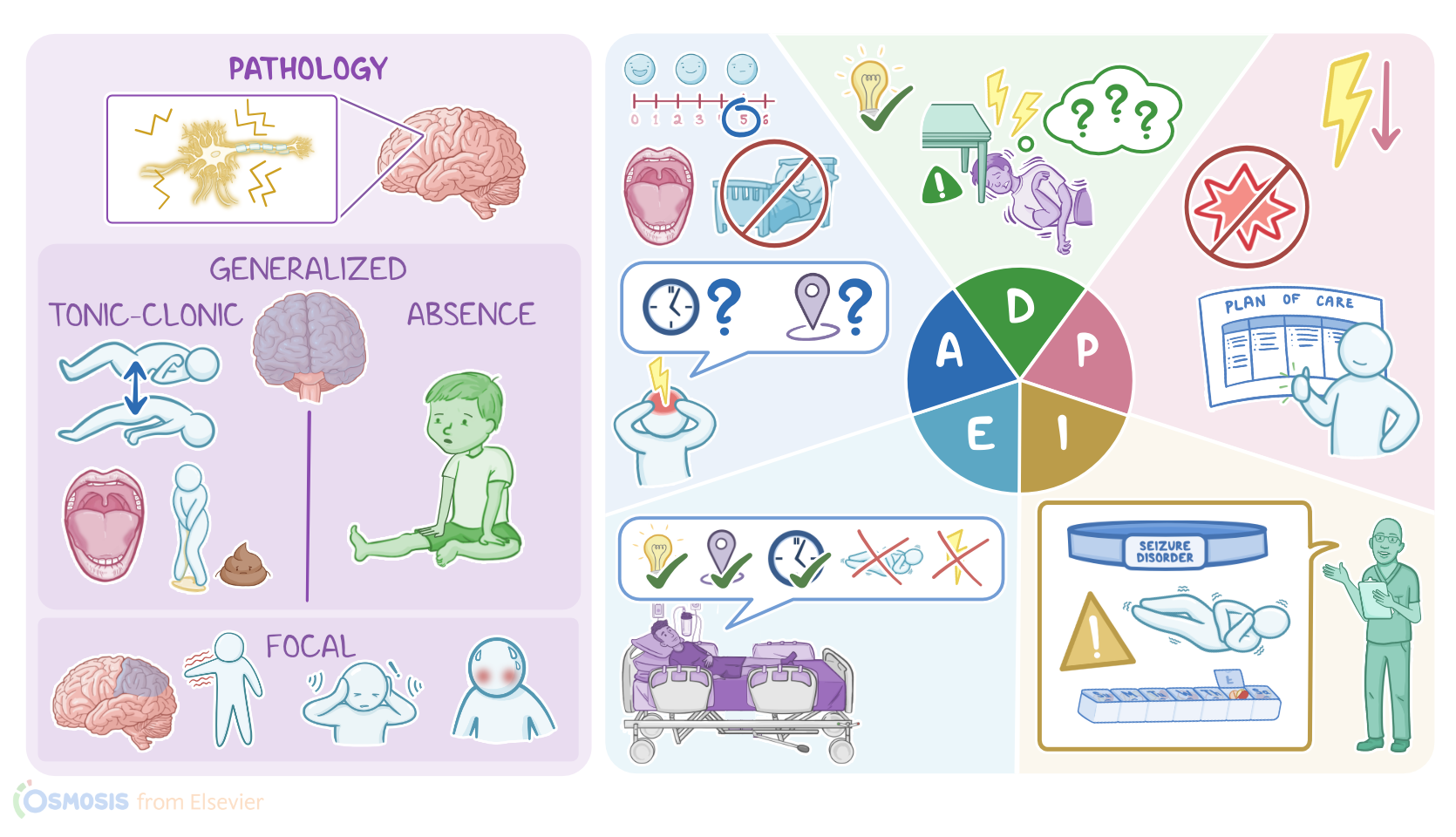
Once the seizure begins, its symptoms depend on the part of the brain involved. So, seizures are classified into two types: generalized and focal.
Generalized seizures arise from both cerebral hemispheres at the same time, and almost always cause a sudden impairment of consciousness, along with motor symptoms that involve the whole body.
The most common subtypes are generalized tonic-clonic and absence seizures. In generalized tonic-clonic seizures, clients experience a tonic phase, where the muscles suddenly tense up, followed by the clonic phase, where muscles rapidly contract and relax.
Contraction of the jaw muscles may cause the client to bite on their tongue. Clients with tonic-clonic seizures may also develop urinary or fecal incontinence.
On the other hand, absence seizures usually occur in children, and they’re characterized by a sudden, brief loss of consciousness without any change in the muscle tone.
So, they could be sitting on their bed or talking to someone and suddenly “space out” or stare blankly into space for a few seconds. Now, in contrast, focal or partial seizures arise from a specific area in one cerebral hemisphere, leading to symptoms that only involve part of the body.
Most often, focal seizures present with motor symptoms, as well as sensory symptoms like a burning or tingling sensation, or hearing or tasting something, and autonomic symptoms like sweating and flushing.
In addition, some clients with focal seizures may lose consciousness. Seizures may be followed by a postictal phase, during which the client’s consciousness is still impaired for minutes to hours, so they may seem sluggish and tired or even hard to wake up.
Another phenomenon that can occur is Todd’s paralysis, which describes a temporary paralysis of the affected extremity. Now, seizures may put the client at risk for physical injuries, such as head trauma, tongue bites, bone fractures, lacerations, and bruises.
These clients are also more likely to develop psychiatric disorders such as depression and anxiety. In addition, clients with epilepsy are often at higher risk of death, which could be due to trauma, suicide, or status epilepticus, which is a seizure that lasts longer than 5 minutes, resulting in permenant brain damage.
Some clients may experience sudden unexpected death in epilepsy, or SUDEP for short, which is when death occurs suddenly, unexpectedly, and for unknown reasons, even in a protected environment like a hospital.
Okay, to diagnose epilepsy, the first step involves taking history and physical examination. Information such as details about the nature of the seizure activity like when the seizure occurred, how long it lasted, what body parts were affected and any events that preceded the seizure.
A brain CT scan or MRI can be done to rule out brain tumors, while an electroencephalogram, or EEG, can be done by placing electrodes on the scalp to monitor the brain’s activity.
Key Takeaways
Seizure disorders may be due to epilepsy, which is a neurological condition characterized by recurrent convulsions that occur due to excessive electrical activity in the brain. Seizures can take many forms, with the most common being generalized tonic-clonic and absence seizures.
In generalized tonic-clonic seizures, people experience a tonic phase, where the muscles suddenly tense up, followed by the clonic phase, where muscles rapidly contract and relax. In absence of seizures which usually occur in children, there is a sudden, brief loss of consciousness without any change in the muscle tone.
The exact cause of epilepsy is often unknown, but it can be due to genetics, brain injury, infections, or developmental disorders, among other causes. The management of seizures involves anti-seizure medications like carbamazepine, phenytoin, and levetiracetam and supportive management.