Endocarditis: Nursing
1,063views
Endocarditis: Nursing
NRS 243
NRS 243
Notes
| ENDOCARDITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Endocarditis refers to inflammation of the inner layer of the heart, called the endocardium. Okay, but first, a bit of anatomy and physiology. The heart wall is made of three layers: the outer layer is the epicardium, the middle layer is the myocardium, and the inner layer is the endocardium. These layers line the four heart chambers, which are the two atria and two ventricles. The endocardium also lines the heart valves at the end of each chamber.
First, there are two atrioventricular valves, the mitral or bicuspid valve on the left, and the tricuspid valve on the right. The atrioventricular valves prevent blood from returning to the atria after filling the ventricles. And second, there are two semilunar valves called the aortic valve at the left, and the pulmonary valve at the right. The semilunar valves prevent blood from returning to the ventricles after being pumped out.
Okay, so depending on its cause, endocarditis can either be infective, or less frequently, non-infective. Infective endocarditis is most often caused by bacteria like Staphylococcus aureus or Staphylococcus epidermidis, which can be found in the skin, and may enter the bloodstream during surgical procedures, or through an infected intravenous catheter, skin wounds, or intravenous drug use.
Another common bacterial cause is Streptococcus viridans, which can be found in the mouth and may enter the bloodstream during a dental procedure. Additionally, Streptococcus gallolyticus is normally found in the intestinal flora; so when there’s colorectal bleeding, like with colorectal cancer, these bacteria can migrate into the bloodstream. On the other hand, Enterococci are a part of the normal urogenital flora, and can enter the bloodstream via genitourinary catheterization or surgery.
Less frequently, infective endocarditis can be caused by the HACEK organisms, which include the bacteria Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, and Kingella. Finally, infective endocarditis can also be caused by certain fungi like Candida albicans; this happens mostly with intravenous drug use or in hospitalized clients who are on multiple antibiotics.
On the flip side, non-infective endocarditis is usually associated with hypercoagulable states, autoimmune diseases like systemic lupus erythematosus, or cancer. The main risk factors for endocarditis include pre-existing heart valve defects, such as mitral valve prolapse, aortic regurgitation, rheumatic heart disease, or having prosthetic heart valves; as well as pre-existing cardiac pathology, such as cardiomyopathy or ventricular septal defects. Additional risk factors include undergoing cardiac surgery, dental procedures, urogenital or central venous catheterization, and IV drug use, as well as older or immunocompromised clients, and those who have an autoimmune disease or cancer.
Now, the pathology of infective endocarditis starts when one of the previously mentioned risk factors causes endocardial damage, which results in local adherence of platelets and fibrin to the damaged area. This creates fertile ground for any potential bacteria to adhere or stick to the damaged endocardium. So, for infective endocarditis to ensue, the client must also develop bacteremia, which is when bacteria manage to enter the bloodstream, and ultimately find their way to the endocardium and settle.
In addition, some bacteria are able to create a biofilm, which is a sticky coating made of sugars and proteins that protects the bacteria from the immune system, and allows them to stick together, forming colonies. These bacterial colonies start collecting clots made of fibrin and immune cells such as leukocytes and form large vegetations.
On the other hand, non-infective endocarditis usually starts with an underlying condition that increases circulating cytokines or antigen-antibody complexes, which settle in the endocardium and cause inflammation. This results in endocardial damage, which exposes the underlying collagen, and in turn causes platelets and fibrin to adhere and form tiny blood clots. Over time, the clots can grow and develop into a sterile vegetation.
Now, these vegetations are large, so they can interfere with the normal function of the heart, causing complications like valve dysfunction, arrhythmias, and in severe cases, heart block and heart failure. In addition, fragments of these vegetations can break off, forming emboli that can escape from the heart into the systemic circulation. These emboli can then lodge in other organs and obstruct blood flow, causing ischemia. When the septic emboli come from the left side of the heart, they can reach the brain, limbs, spleen, and kidneys; while right-sided emboli typically reach the lungs.
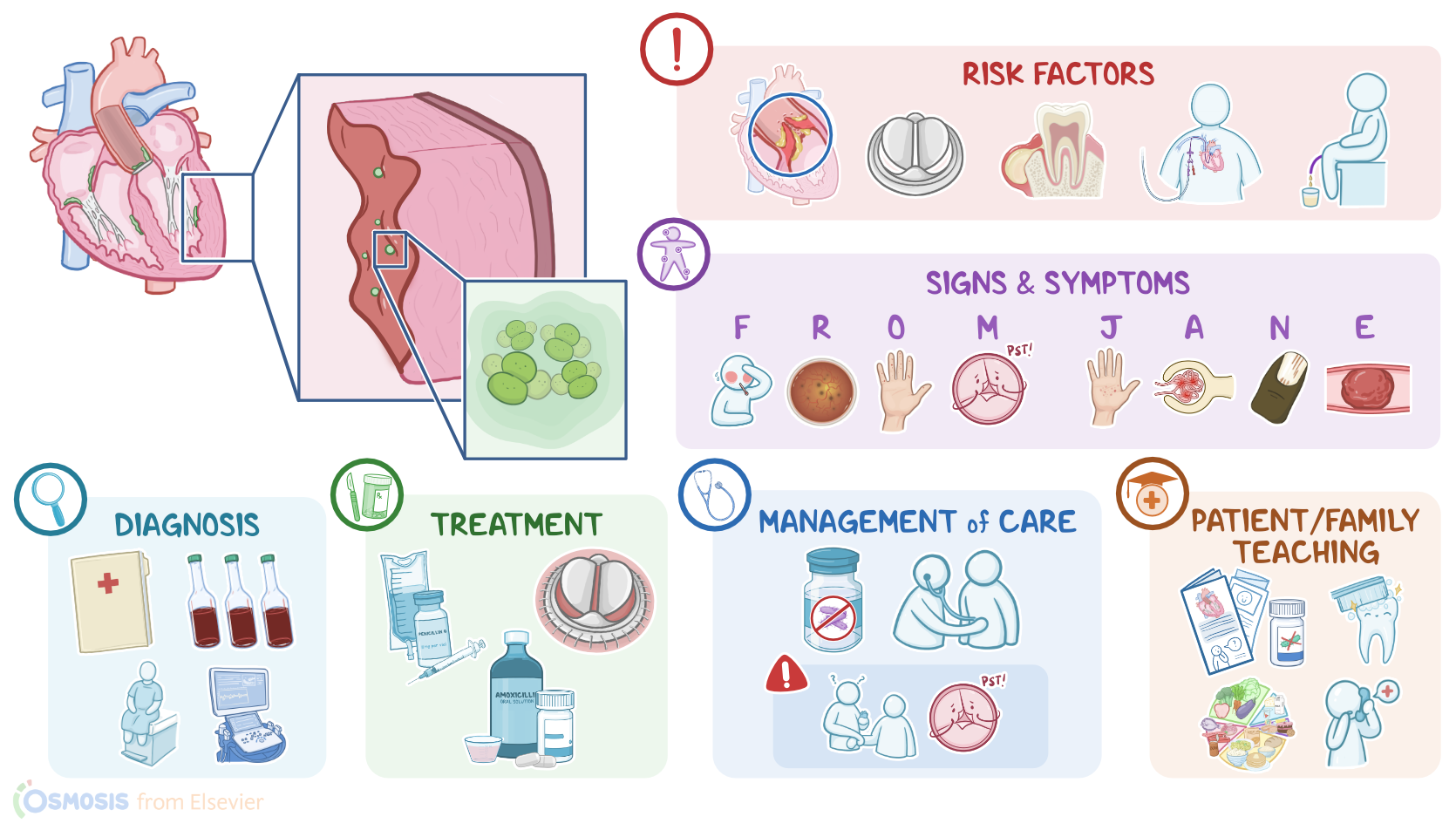
Okay, the main clinical manifestations of endocarditis often include fever, chills, and fatigue; as well as a new systolic murmur that results from turbulent blood flow past the damaged heart valve. Sometimes, emboli can detach from the valve to float through the bloodstream. The emboli can then lodge under the nail-bed, causing splinter hemorrhages that look like black longitudinal streaks underneath the nail; or can lodge in the palms and soles, causing small painless, flat, and red lesions, called Janeway lesions.
In addition, there might be an immune reaction with antigen-antibody complexes that form and deposit in different parts of the body; in the fingers and toes, these complexes can lead to painful, red, raised lesions called Osler nodes; whereas in the eye, they may lead to Roth spots, which are hemorrhagic spots on the retina.
Finally, the deposits can reach the kidney, leading to acute glomerulonephritis. Emboli from endocarditis can also cause more serious complications, including intestinal ischemia, pulmonary embolism, and stroke. These clinical manifestations can be remembered with the mnemonic FROM JANE, which stands for Fever, Roth spots, Osler nodes, Murmur, Janeway lesions, Acute glomerulonephritis, Nail-bed hemorrhage, and Embolism.
Additionally, come clients may develop complications of endocarditis and valve dysfunction, such as heart failure, which presents with fatigue, tachycardia, and dyspnea, as well as edema.
Diagnosis of endocarditis starts with the client’s history and physical assessment; followed by laboratory tests, where three blood cultures should be obtained in an hour, from three different sites.
However, some bacteria and fungi won’t grow on normal cultures or, if antibiotics have been used in the two weeks previous to obtaining the cultures, because they may inhibit bacterial growth, causing false negative results. Blood tests usually show mild leukocytosis, as well as increased inflammatory markers ESR and CRP. Transesophageal echocardiography can also be used to visualize the heart and look for vegetations or abnormal valve movement.