Inflammatory bowel disease - Crohn disease and ulcerative colitis: Nursing
2,418views
Inflammatory bowel disease - Crohn disease and ulcerative colitis: Nursing
MS LEC PRELIMS 2nd SEM
MS LEC PRELIMS 2nd SEM
Notes
| INFLAMMATORY BOWEL DISEASE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
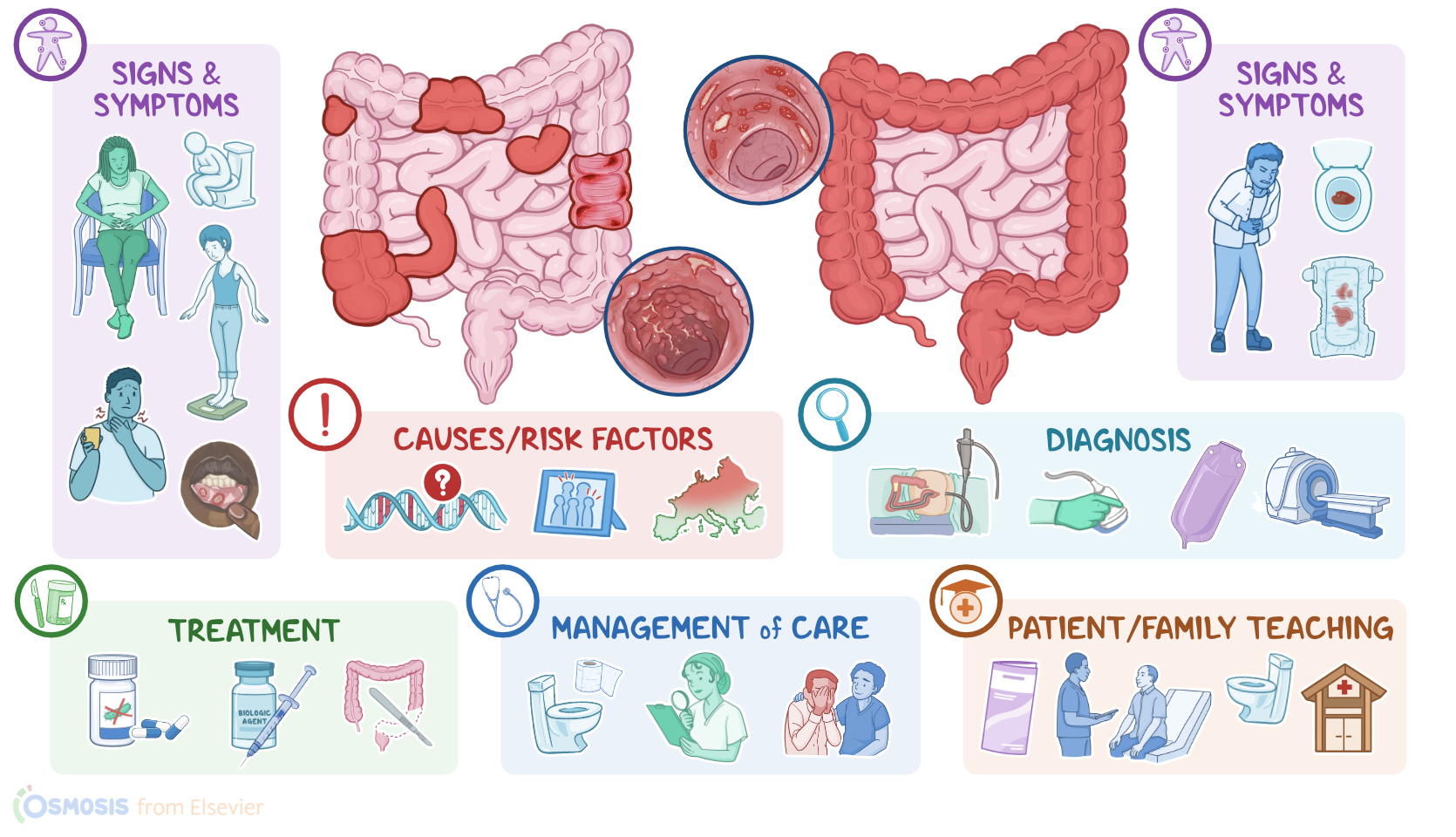
Inflammatory bowel disease or IBD is a condition characterized by chronic gastrointestinal tract inflammation due to autoimmune reactions, as well as systemic symptoms like fatigue, fever, and unintentional weight loss. There are two types of IBD, Crohn disease and ulcerative colitis.
The gastrointestinal tract consists of a long tube, where food travels through, which runs from the mouth to the anus.
Now if we zoom into a cross-section of the gastrointestinal tract, the walls are typically lined by the same four layers of tissue. From the inside out, there’s the mucosa, which absorbs nutrients and secretes mucus and digestive enzymes; the submucosa, a dense layer of tissue that contains blood vessels, lymphatics, and nerves; the muscularis externa, which contracts to move food through the bowel; and the outermost layer is either the adventitia or the serosa, and faces the abdominal or peritoneal cavity.
So when we eat a big meal, the food travels from the mouth, down the pharynx and esophagus, to reach the stomach, which has a handful of glands that secrete hydrochloric acid and pepsin to help digest the food, now called a bolus.
Then the bolus passes towards the small intestine, or small bowel, made of the duodenum, jejunum, and ileum, where nutrients are absorbed. Examples are - monosaccharides, amino acids, fatty acids, electrolytes, minerals, vitamins, and water.
To increase the surface for absorption, the mucosa in the small intestine has lots of tiny ridges and grooves, each of which has little finger-like projections called villi. And in turn, each villus is covered in tiny little microvilli. Then, whatever isn’t absorbed travels to the large intestine, made of the cecum, colon, rectum, and anal canal.
Here, there are trillions of bacteria, collectively called the gut microbiome, which help produce essential B and K vitamins. Now, in the large intestine, a little more water and electrolytes are absorbed to finally form the feces that are eliminated through the anus.
Now, the exact cause of IBD is unknown, but there’s a genetic component because it runs in families. So, risk factors include family history, northern European descent, and the presence of genetic and inflammatory disorders like cystic fibrosis, psoriasis, or multiple sclerosis.
In addition, smoking and Ashkenazi Jewish descent are associated with an increased risk for Crohn disease.
Now, the pathology of inflammatory bowel disease starts in the gastrointestinal tract of a genetically susceptible client when the immune system is triggered by an antigen. initiating an excessive inflammatory response. This ends up damaging the mucosal epithelium, which provides a perfect environment for bacteria to invade and grow.
More immune cells come to the scene, and release cytokines, that cause further inflammation and damage. In Crohn disease, the inflammation can occur anywhere from the mouth to the anus.
They appear most commonly in the terminal ileum and colon, but usually spares the rectum. There’s typically large areas of healthy tissue in between damaged areas, so they’re called “skip lesions.”
The lesions caused by the inflammation involve the entire depth of the intestinal wall, which is referred to as being transmural. These deep lesions and ulcers often run longitudinally along the tissue with sections of normal mucosa in between, thus creating a “cobblestone” appearance.
On the flip side, with ulcerative colitis, the inflammation most often starts at the rectum, and spreads continuously along the large intestine. The damage is limited to the mucosa and submucosa of the intestinal wall. Over time, both Crohn disease and ulcerative colitis may lead to several complications.
With both Crohn disease and ulcerative colitis, there might be acute or chronic bleeding and anemia due to iron deficiency. Sometimes, a phlegmon can form, which is where there’s a localized area of inflammation in the intestinal wall that can get infected and become an abscess.
Now Crohn disease can result in strictures, which may eventually cause bowel obstruction. Other complications include micro-perforations and fistulas, which are communications between two epithelial organs.
If the small intestine is affected, there’s reduced absorption of bile salts which increases the risk of gallstones.
Decreased fat absorption will cause the excess fat to bind to calcium in the small intestine. This prevents oxalate from binding to the calcium so they’re absorbed into the body and increase the risk of developing calcium-oxalate kidney stones.
Now, ulcerative colitis is more likely to cause toxic megacolon as a complication but this could also occur in Crohn disease. This is where the nerves and muscles are damaged and the colon becomes atonic and dilated. This results in stool build up and the colon becomes dilated. In severe cases, it can lead to perforation with peritonitis.
Other conditions that often occur with ulcerative colitis include inflammatory arthritis, such as ankylosing spondylitis, skin lesions like pyoderma gangrenosum and erythema nodosum, as well as primary sclerosing cholangitis, which is when there’s fibrosis and inflammation of both the intra- and extrahepatic bile ducts.
Finally, clients with inflammatory bowel disease are at increased risk for developing colorectal cancer.
In Crohn disease, gastrointestinal symptoms include crampy abdominal pain, watery diarrhea that may or may not be bloody, and sometimes malabsorption symptoms like steatorrhea, or B12 deficiency, causing malnutrition as well as weight loss.
A very frequent finding are aphthous ulcers in the mouth. Some clients may also present esophageal involvement, with odynophagia or painful swallowing, and dysphagia.
Clients with ulcerative colitis usually present with gastrointestinal symptoms that include colicky abdominal pain, which is often relieved after defecation; bloody diarrhea; rectal bleeding; and tenesmus, which is pain when defecating. There may also be malaise, anorexia, and fever.
All right, diagnosis of IBD starts with the client’s history, and physical assessment, followed by endoscopy or colonoscopy with biopsy to confirm the diagnosis. Laboratory tests may also show elevated ESR or PCR and fecal calprotectin, which indicate an inflammatory process in the gastrointestinal tract.
Finally, imaging studies like barium enema, ultrasound, CT, and MRI can be performed to assess the extent of inflammation in and beyond the bowel wall.
Now, the choice of treatment depends on the type and severity of IBD. Usually, treatment involves the use of corticosteroids, methotrexate or 5-aminosalicylic acid, or 5-ASA for short.
An alternative is antibiotics like ciprofloxacin and metronidazole, which are thought to help control symptoms by reducing bacteria levels in the intestine and by curbing the immune response.