Polycythemia: Nursing
Polycythemia: Nursing
Acute Final
Acute Final
Notes
| POLYCYTHEMIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
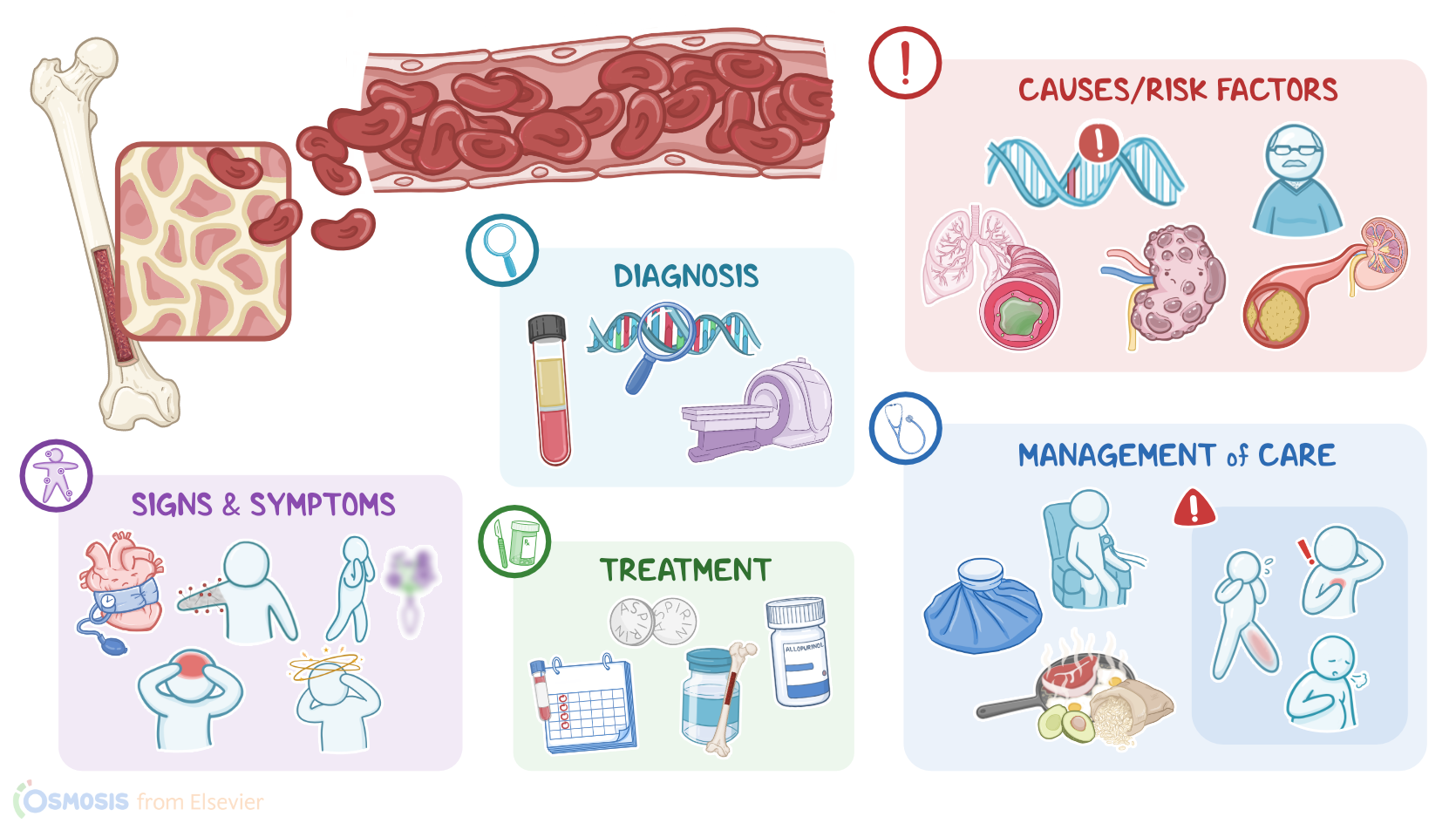
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| COMPLICATIONS |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Polycythemia is a condition associated with an increased number of circulating red blood cells or RBCs for short.
Polycythemia can be primary, meaning there's a spontaneous increase in the production of red blood cells; or secondary, when another condition causes increased production.
First, let’s cover some basic physiology of blood cells, starting with RBCs. When we breathe in, air flows through the nasal cavity, pharynx, and larynx, down into the trachea. From here, the air reaches the lungs, where RBCs pick up oxygen and transport it to the peripheral tissues, where they release it.
After releasing oxygen, the RBCs pick up carbon dioxide.
Carbon dioxide is a waste product of cellular metabolism,
which is then transported back to the lungs,
and eventually eliminated through the air that we breathe out.
Additionally, red blood cells have an important role in maintaining the acid-base balance in the body.
The production of red blood cells starts in the bone marrow, where the hematopoietic stem cells reside.
In order to proliferate and reach their mature form, hematopoietic cells require stimulation by specific growth factors. One of these factors is a hormone called erythropoietin, produced by kidneys. Once produced, erythropoietin enters the blood and travels to the bone marrow, where it signals hematopoietic cells to differentiate into red blood cells.
Moreover, if there’s tissue hypoxia or low levels of oxygen in peripheral tissues, the kidneys can increase the production of erythropoietin, therefore ramping up the production of red blood cells.
Finally, the other two groups of blood cells include white blood cells, which primarily defend the body from foreign pathogens; and platelets, which have a key role in blood clotting and hemostasis.
Now, primary polycythemia, also known as polycythemia vera, is a chronic myeloproliferative disorder caused by an acquired mutation of the JAK2 gene, which codes for a protein that promotes cell growth and proliferation.
Risk factors associated with this mutation include being assigned male at birth and over 50 years of age.
On the other hand, secondary polycythemia is usually caused by conditions associated with tissue hypoxia, like high altitude, chronic obstructive pulmonary disease, and cyanotic heart disease.
Other important causes include renal conditions, like renal artery stenosis, renal cysts, and renal tumors;
Next are erythropoietin secreting tumors, like hepatocellular carcinoma.
Finally, some medications like erythropoietin analogs, testosterone, and anabolic steroids can cause polycythemia as a side effect.
Risk factors associated with secondary polycythemia include smoking, obesity, chronic alcoholism, and hypertension.
Now, let’s switch gears and look at the pathology of polycythemia. In primary polycythemia, the mutation of the JAK2 gene causes hematopoietic cells to divide even in the absence of erythropoietin. As a result, there’s overproduction of primarily red blood cells, but also white blood cells and platelets.
On the other hand, with secondary polycythemia, tissue hypoxia stimulates the production of erythropoietin, which increases the production of red blood cells, eventually causing polycythemia.
In both types of polycythemia, the increased the volume and viscosity of the blood ultimately causes sluggish blood flow, congestion in the peripheral organs,
and tissue hypoxia and ischemia.
Now, complications of polycythemia are primarily linked to increased viscosity of the blood and circulatory congestion, because these factors increase the risk of developing blood clots or thrombosis.
The most common thrombotic complications include stroke, angina pectoris, myocardial infarction, and deep vein thrombosis.
Additionally, high turnover of red blood cells is characterized by increased levels of uric acid in the body, which can result in complications such as kidney stones and gout, which is a type of joint inflammation caused by high levels of uric acid.
Other important complications include peptic ulcers, hepatomegaly, and splenomegaly. Moreover, splenomegaly occurs because the spleen is trying to eliminate the excess blood cells from circulation.
Now, the clinical manifestations of polycythemia are often caused by blood vessel congestion.
When cerebral circulation is affected, there’s dizziness and headaches; retinal vessel congestion causes blurred vision;
impaired peripheral circulation can cause tingling or burning in the hands and feet; additionally, when there’s pain, swelling and redness in the hands and feet, it’s called erythromelalgia and this can be triggered by stress, exercise, temperature change, or dehydration.
There can also be facial plethora which is ruddy complexion.
Another common symptom is pruritus, or itchiness, especially after a hot shower or bath, and this is likely due to overproduction of histamine and prostaglandins by mast cells. There can also be systemic effects, like fatigue, from a combination of hypoxia and iron deficiency.