Hypopituitarism: Nursing
Hypopituitarism: Nursing
Acute Final
Acute Final
Notes
| HYPOPITUITARISM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
With hypopituitarism, hypo- means low and pituritism refers to the pituitary gland. So hypopituitarism describes an excessive decrease or absence of the pituitary hormones. Now, hypopituitarism comes in two flavors: selective hypopituitarism, meaning only one pituitary hormone is deficient, and this is the more common scenario; and panhypopituitarism, a rare situation when all pituitary hormones are deficient, which can be life threatening.
Now, the pituitary is a small, pea-sized gland at the base of the brain. Specifically, the pituitary gland sits in the sella turcica, a small bony cavity in the sphenoid bone. This is really just a fancy way to say “behind the nose!” Above the pituitary gland, there’s the optic chiasm, and laterally, there are the cavernous sinuses. Now, let’s quickly review some anatomy and physiology.
The pituitary gland is made up of an anterior lobe and posterior lobe. The anterior lobe, also called the adenohypophysis, contains endocrine cells that produce tropic hormones, which in turn control the secretion of hormones from other endocrine glands or influence a response in target tissues. These include thyroid stimulating hormone, or TSH; adrenocorticotropic hormone, or ACTH; growth hormone, or GH; the gonadotropins, namely follicle stimulating hormone, or FSH, and luteinizing hormone, or LH; prolactin. Additionally, a smart part of the pituitary gland that can be considered part of the anterior lobe secretes melanocyte stimulating hormone, or MSH.
So for the anterior lobe, TSH stimulates thyroid hormone production, which, in turn, increases the basal metabolic rate in all cells. Next, ACTH stimulates adrenal cortisol production, which, in turn, has plenty of effects around the body, such as regulating glucose metabolism, blood pressure, and electrolyte balance, and immunity.
Then there’s GH, which stimulates the growth and development of various body tissues, and it also causes release of insulin like growth factor 1 or IGF1, from the liver and skeletal muscles, which mediates the effects of GH on target tissues. Finally, prolactin stimulates lactation during breastfeeding; while FSH and LH influence the function of gonads. Specifically, FSH stimulates the production of ova in the ovaries and the production of sperm in the testes; while LH stimulates ovulation and the secretion of sex hormones, estrogen and testosterone, in both assigned males and females at birth. All of these hormones are regulated via negative feedback. This means that when a gland, say, the thyroid, secretes more thyroid hormones, that inhibits TSH levels, in order to bring balance back to the endocrinology realm.
The posterior lobe, on the other hand, contains hormone-secreting nerve endings extending down from the hypothalamus. The posterior lobe secretes antidiuretic hormone, also called vasopressin or simply ADH, which regulates fluid volume in the body by promoting the reabsorption of water from the urine in the kidneys, making it more concentrated, and it also works as a potent vasoconstrictor. Next is oxytocin, which stimulates uterine contractions during childbirth and causes the breast to push down milk during breastfeeding.
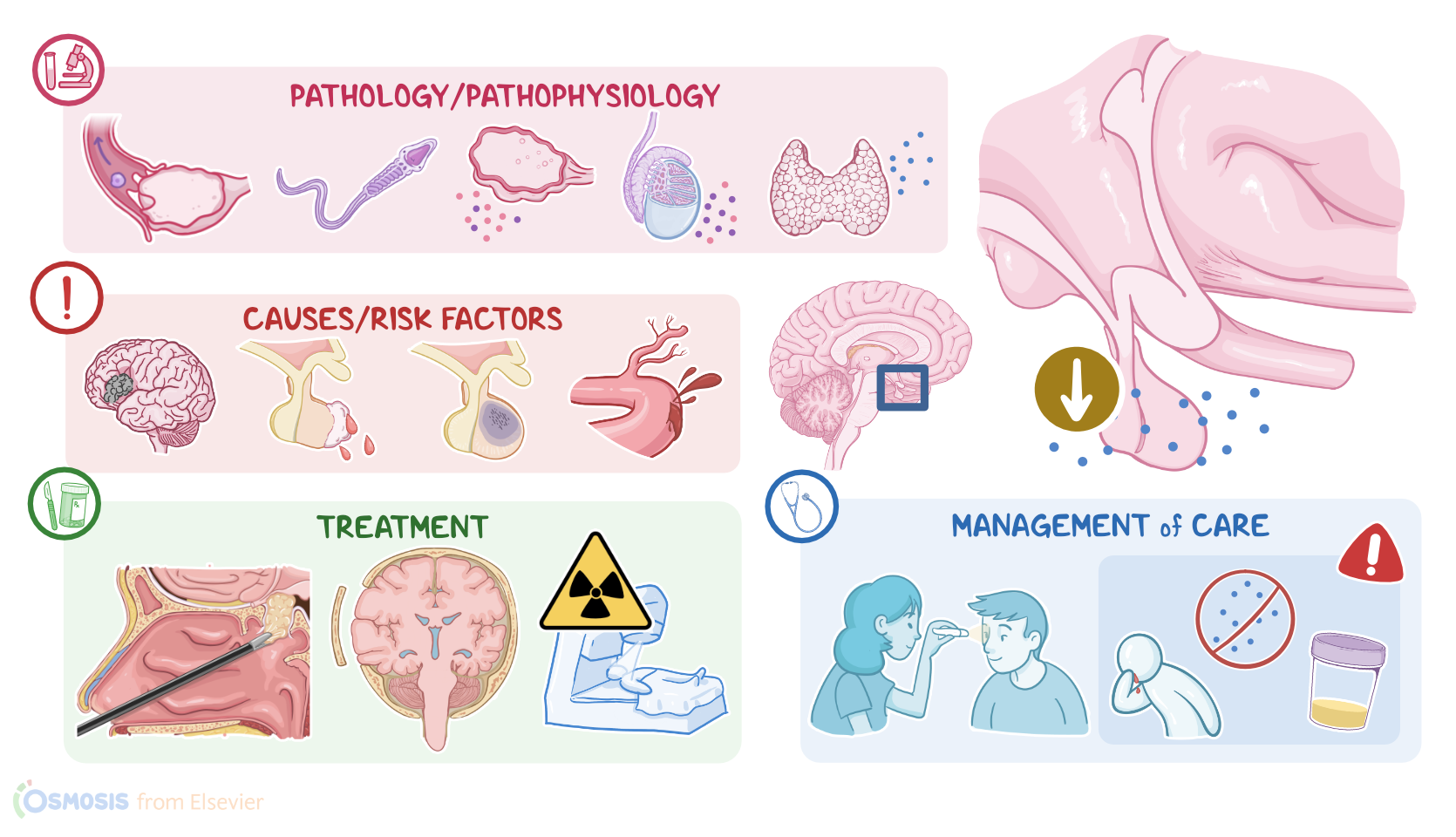
Alright, now the most common cause of hypopituitarism are pituitary adenomas, which are benign tumors of the pituitary gland. Such tumors can sometimes bleed spontaneously, and this is called pituitary apoplexy. Alternatively, a brain stroke can cause a drop in the blood supply to the pituitary gland, and this is called pituitary infarction. Pituitary function can also be impaired as a consequence of malnutrition or rapid weight loss.
In addition, postpartum hemorrhage can cause a sudden drop in blood and oxygen supply to the pituitary, damaging it, and this cascade of events is called Sheehan’s syndrome. Other causes of hypopituitarism include head trauma, brain tumors or infections, radiation or surgery to the head and neck, and can also occur during the last stages of HIV disease. Finally, if the cause of hypopituitarism is unknown, it’s called idiopathic hypopituitarism.
Now, let’s switch to risk factors for hypopituitarism, which include traumatic brain injury, cocaine use, subarachnoid hemorrhage, postpartum hemorrhage and hypotension, which can progress to Sheehan’s syndrome. Blacks also have an increased incidence of pituitary tumors, so they’re at increased risk of developing hypopituitarism. Regardless of cause, hypopituitarism causes decreased secretion of target gland hormones, which in turn reduces their effects in the body.
ACTH deficiency causes adrenal insufficiency, which means the adrenal glands produce less cortisol. This impairs glucose metabolism, causing hypoglycemia. Decreased cortisol levels can also cause loss of peripheral vascular tone, which means that the arteries can’t narrow appropriately in order to raise blood pressure. This results in hypotension, tachycardia and can progress to vascular collapse and renal insufficiency because of insufficient blood flow to the kidneys.
On the other hand, decreased TSH levels decrease thyroid hormone production, which lowers the basal metabolic rate of all body cells. With decreased gonadotropins, there’s decreased sex hormone production, which can cause loss of secondary sexual characteristics, as well as like decreased sperm production and infertility, or anovulation and infertility. Finally, growth hormone deficiency causes reduced production of IGF-1 from the liver. As a consequence, bones aren’t stimulated to renew when osteoclasts decrease the amount of bone matrix. This leads to decreased bone density, called osteoporosis, which in turn increases the chance of pathological fractures.
Clients with hypopituitarism typically present with signs and symptoms related to the deficient hormone. Clients with ACTH deficiency can present with headache, fatigue, anorexia and decreased body hair, in addition to hypotension, tachycardia, and shock, which could be life threatening without cortisol replacement. With TSH deficiency, there can be alopecia, lethargy, weight gain, intolerance to cold, and bradycardia. Clients with growth hormone deficiency can have decreased muscle strength, increased cholesterol levels, and decreased bone marrow density.
Next, with gonadotropin deficiency, clients typically can present decreased facial and body hair, decreased muscle mass and bone density, decreased libido, erectile dysfunction, and amenorrhea. Moreover, pituitary adenomas can cause compression symptoms such as headache, projectile vomiting, as well as visual disturbances due to compression on the optic chiasm.
Finally, it’s worth mentioning that ADH deficiency can occur following surgical treatment of a pituitary adenoma. This causes a rare condition called diabetes insipidus. Although it’s called diabetes, it has nothing to do with blood sugar levels. Clients with diabetes insipidus typically present with signs and symptoms of increased urine output. These include dehydration and thirst, hypotension, increased plasma osmolarity, and irregular plasma electrolyte levels. These clients may also have low urine specific gravity of less than 1.005, which is characteristic of diabetes insipidus.
The diagnosis of hypopituitarism starts with the client’s history and medical assessment, followed by laboratory tests. These tests include direct and indirect measurements of pituitary hormone levels, such as TSH, ACTH, FSH, LH, GH and prolactin, which can show a decrease in one or all of these hormones. Target gland hormones, like free thyroid hormones, FT3 and FT4; cortisol; estrogen, progesterone and testosterone, can also be low. CT scans and MRI can also be used to identify enlargements, erosions, or calcifications, which are markers for pituitary tumors. Finally, an angiogram can be done to rule out vascular issues, like strokes or aneurysms.
Finally, the treatment of hypopituitarism may be grouped into surgical and non-surgical options. Pituitary adenomas can be surgically removed, usually by removing the entire pituitary gland, called a hypophysectomy; and this is usually done through transsphenoidal resection, which is when the tumor is taken out through the nose. Alternatively, some tumors can be removed through a craniotomy, when the skull is opened to access brain structures.