Physiology of pain: Nursing
2,799views
Physiology of pain: Nursing
Watch later
Watch later
Notes
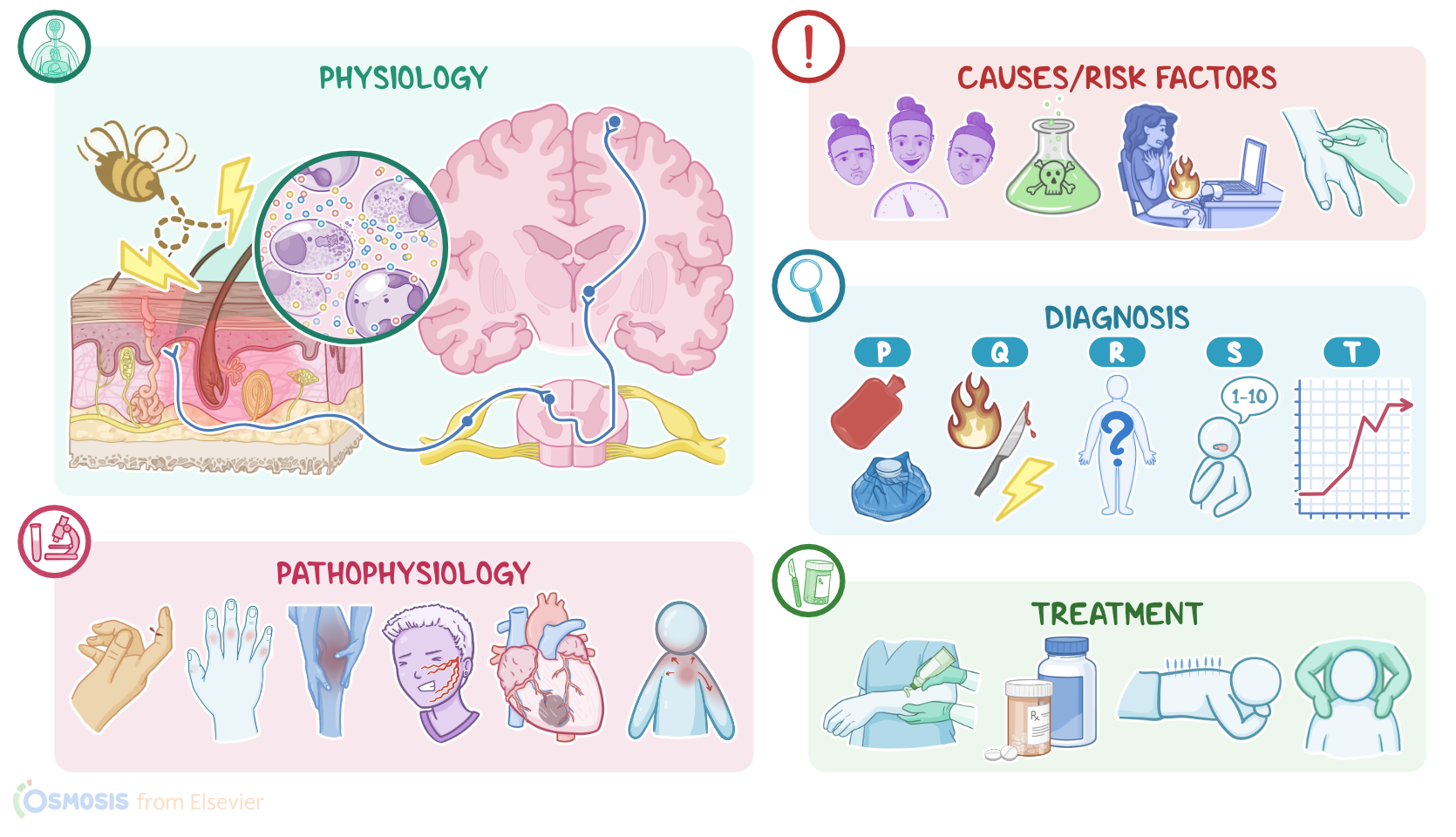
| PHYSIOLOGY OF PAIN | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
Transcript
Pain is an unpleasant physical or emotional experience that occurs in response to actual or potential tissue damage. Depending on the cause and duration, pain can cause suffering and decreased quality of life. As a symptom, pain is one of the most common reasons that bring clients to healthcare facilities.
First, let’s look at the four main mechanisms involved in the physiology of pain, which are transduction, transmission, perception, and modulation. Transduction is the process through which a pain-inflictive stimulus is converted into a biological signal. This stimulus can be mechanical, like pinching someone; chemical, like a strong acid causing chemical damage to the skin; or thermal, like spilling hot coffee on your lap. Now, these situations cause the damaged tissue, and in the case of inflammation, nearby immune cells to release molecules that can trigger pain like serotonin, histamine, prostaglandins, bradykinin, and substance P. These will activate special pain receptor cells called nociceptors and cause them to fire off an action potential. Think of this as a message that tissue injury has occurred.
Now, after the action potential has been generated, the second step begins, which is transmission of the action potential from the site of injury to the cortex of the brain. The nociceptors are first order neurons, and they relay the action potential to the dorsal horn of the spinal cord where they synapse with a second order neuron. The second order neuron carries the message up to the brainstem and thalamus where they synapse with a third order neuron. The third order neuron is responsible for carrying the message to the cortex for processing.
Once the message reaches the cortex, specifically the somatosensory cortex, the next step called perception begins. This is where you consciously perceive pain and its characteristics like location, intensity, and what makes the pain better or worse. Different regions of the somatosensory cortex correspond to different parts of the body and those parts with more nociceptors like the face and hands, take up a larger portion of the cortex, so you end up with a sensory homunculus mapped onto the somatosensory cortex.
Additionally, during pain perception, an emotional response is triggered, and this is often a negative emotion like anger or fear. This is helpful since it leads to an immediate behavioral response where you move away from the stimuli that’s causing the pain; for example, moving away from the person pinching you, or wiping the hot coffee off your leg.
And finally, pain modulation refers to how the pain signal is altered along the nervous pathways, thanks to descending modulatory fibers that travel from the brain down to the spinal cord. These can be stimulatory or inhibitory depending on whether they release chemical signals that enhance the perception of pain or diminish it. This allows factors like emotion to have a modulatory effect on pain so for example, even though childbirth is an extremely painful event, in some cases, the pain is perceived as less intense because the birth giver feels that having a baby is positive and desired.
Okay, now, pathology-wise, pain can be classified by its duration, like acute and chronic pain; as well as by its type, into nociceptive, neuropathic, ischemic, and referred pain.
Acute pain has a sudden onset and is time-limited, typically resolving within 3 months. This can be trauma like cutting your finger, a disease like kidney stones, an infection like a dental abscess, or acute ischemia like a heart attack. Symptoms of acute pain include manifestations of sympathetic nervous system stimulation, like tachycardia, increased blood pressure, sweating, or dilated pupils. Acute pain is also typically well localized, and clients can usually pinpoint its location. Acute pain is unpleasant, but useful, because it can warn the person about potential or actual tissue damage.
Chronic pain, on the other hand, has a more gradual onset, and is mainly caused by long-term or chronic disorders such as endometriosis, rheumatoid arthritis or Crohn disease, to name a few; and the pain lasts more than 6 months. Chronic pain usually doesn’t result in symptoms of sympathetic nervous system stimulation, because it eventually becomes desensitized to the input from nociceptors. Chronic pain can negatively impact the function of the affected tissue, as well as the client’s long-term psychological well-being and quality of life.
Next, let’s look at the various types of pain. Nociceptive pain focuses on what kind of tissue is damaged, and this can be either somatic or visceral. Somatic pain typically comes from skin, bones, joints, and connective tissue. It usually has a throbbing or aching quality, and it is well localized, meaning a person can often pinpoint where the pain is coming from. Common examples of somatic pain include pain from an arthritic knee or a toothache.
Visceral pain comes from organs like those in the gastrointestinal tract and can result from inflammation, ischemia, stretching, or occlusion; like with hepatitis, there’s liver inflammation, which makes the liver swell and distend the tissues surrounding it, that respond by eliciting a pain signal. In contrast to somatic pain, visceral pain is often diffuse and not well localized.