Bladder exstrophy: Nursing
Bladder exstrophy is a congenital malformation where the bladder protrudes outside of the abdomen due to an abdominal wall defect.
First, let’s quickly review the embryological development of the bladder. The renal system, including the bladder, starts developing during week 4 of intrauterine life. At that point, the embryo is made up of three primitive germ layers: the ectoderm, the mesoderm and the endoderm. Towards the end of week 4 of development, the endoderm in the hindgut, which is the last portion of the primitive digestive tract, begins to expand forming the cloaca. The cloaca is a temporary structure connecting the urinary, digestive, and reproductive ducts.
By week 7, a wall of tissue called the urorectal septum forms in the cloaca and splits it into a posterior anorectal canal for the digestive tract, and an anterior urogenital sinus for genital and urinary structures. And the top portion of the urogenital sinus stretches out to form the primitive bladder. Ultimately, the cloacal membrane opens to the outside of the body for these structures to have openings. Now, at around the same time in development, the muscles and connective tissue of the lower anterior abdominal wall also begin to form.
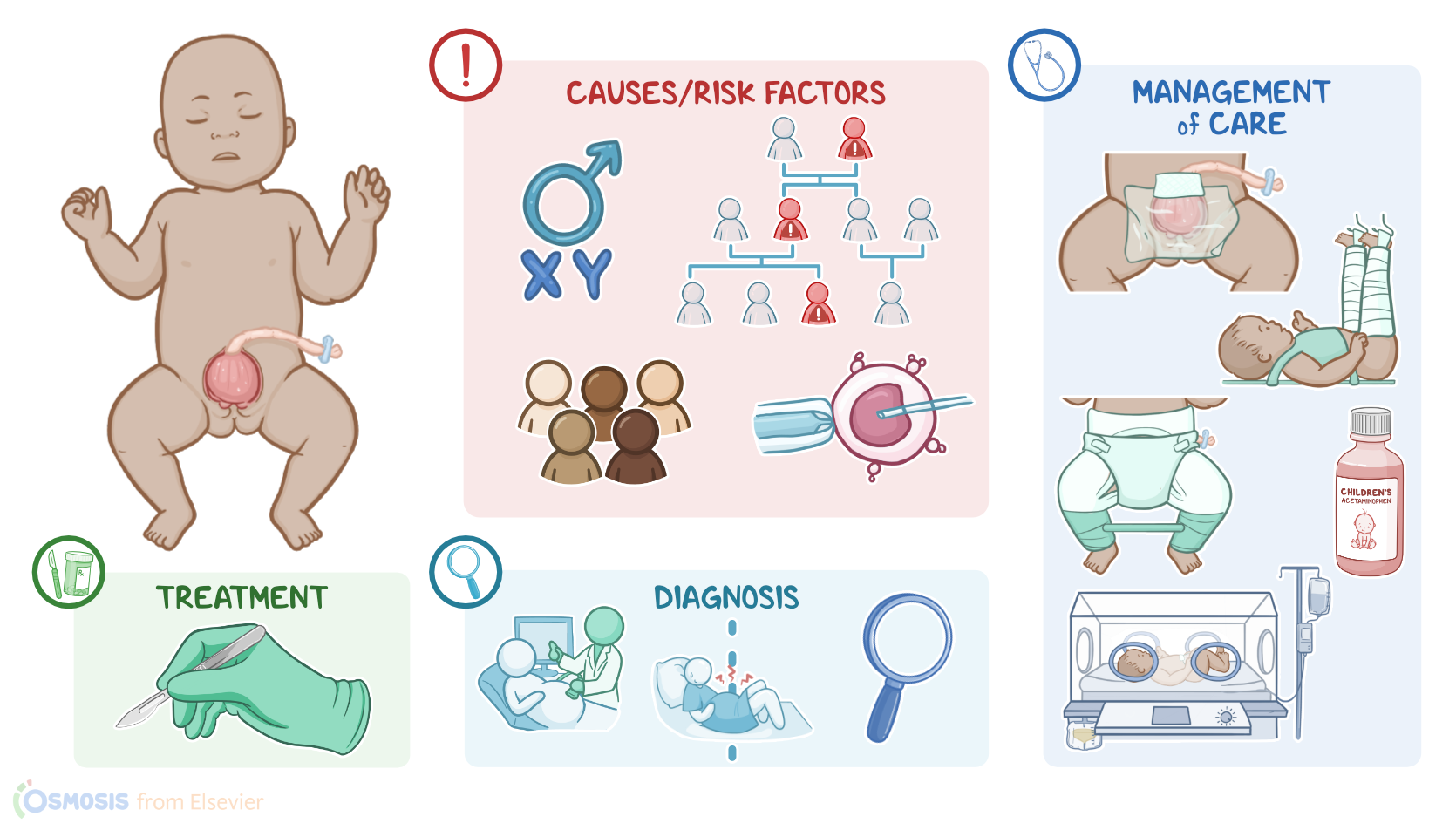
Alright now, bladder exstrophy occurs when there is a midline closure defect during fetal development. Although the exact cause remains unknown, several risk factors have been identified. These include having a family history of bladder exstrophy, being white, or being assigned male sex at birth. This condition is also more common in infants born through assisted reproductive technology, such as in vitro fertilization, or IVF.
Now, when it comes to pathology, the most widely accepted theory for how bladder exstrophy occurs is that the cloacal membrane grows too much, and pushes towards the front of the embryo like a wedge. This prevents the normal midline closure of the abdominal wall. Subsequently, the cloacal membrane ruptures, which renders lower abdominal structures, like the bladder, open and exposed outside of the lower abdominal wall. This also affects the development of other lower abdominal structures, including the symphysis pubis, genitalia and anus.
Okay, now bladder exstrophy can lead to several complications, including urinary incontinence and an increased risk of urinary tract infections. It can also lead to sexual dysfunction and an increased risk of bladder cancer.
Now, individuals with bladder exstrophy present with the inside of the bladder being outside of the abdomen. The bladder is also usually flat instead of its typical rounded shape. Since the bladder is open, urine often drips from the open bladder rather than through the urethra. Individuals with bladder exstrophy can also have a low-set umbilicus; diastasis of the symphysis pubis, meaning this joint is often wider than normal; and an anteriorly displaced anus, where the anal opening is placed more towards the front.
Other genital malformations are also commonly present. In assigned males at birth, these can include a shortened penis and epispadias, which is when the urethra opens on the dorsal side, or on top of the penis. In assigned females at birth, genital findings can include a bifid clitoris or an anteriorly displaced vaginal opening.
Diagnosis of bladder exstrophy can start prenatally with ultrasound can show absence of bladder filling, pubic bone diastasis, a low-set umbilicus and smaller than average genitalia for gestational age. After birth, diagnosis is diagnosed clinically through observation.
Treatment of bladder exstrophy focuses on surgically closing the abdominal wall defect and it is usually done within the first days or weeks of life. However, sometimes, staged surgeries are necessary over months or years.
Alright, let’s look at the nursing care you’ll be providing for a newborn with bladder exstrophy. Your priority goals of nursing care are to protect the exposed bladder and monitor for complications after surgery.
Immediately after delivery, focus on protecting the exposed bladder by covering the bladder with a non-adherent dressing to minimize heat and fluid loss and to keep it moist and protected from germs or debris.
| BLADDER EXSTROPHY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below